



AI scribes now draft therapy notes in seconds, promising freedom from that growing pile of paperwork. But can algorithms truly capture the intensity of a session? Three concepts separate documentation from connection: risk, rupture, and repair. AI is good at detecting explicit risk markers, yet it fails to document ruptures and repairs, which unfold through silence, hesitation, and shared vulnerability. Without clinical inference, AI risks flattening relational nuance into false certainty. This article outlines what AI therapy notes should and should not capture, ensuring notes remain both efficient and clinically safe.
The Three Pillars of Clinical Documentation
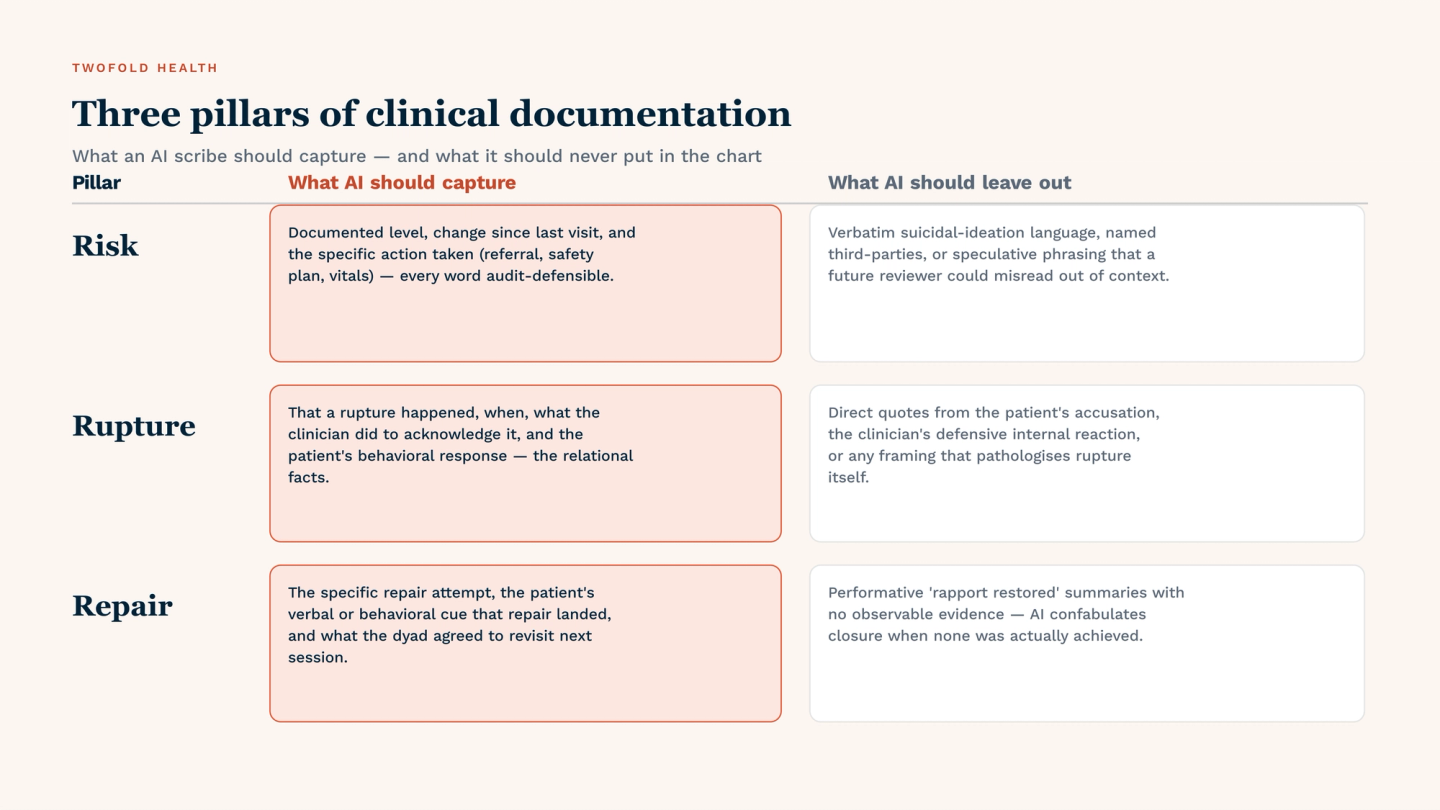
Effective therapy notes rest on three distinct clinical pillars: risk, rupture, and repair. Each places different demands on documentation, and each interacts with artificial intelligence in unique ways:
1. Risk
Risk documentation typically includes suicidal ideation (with or without plan/intent), homicidal thoughts, self‑harm behaviors, substance use relapse, and indicators of child or elder abuse. These are high‑stakes entries that must be precise, timely, and actionable.
AI’s Strength:
AI excels at pattern recognition in unstructured text. Natural language processing (NLP) models can rapidly flag phrases such as “I hurt myself again.” This speed allows clinicians to review flagged content without re‑reading entire transcripts.
Risk Documentation: AI vs. Human Clinician
Documentation Element | AI Capability | Human Clinician |
|---|---|---|
Frequency of risk-related keywords | Excellent; rapid flagging | Slower but contextual |
Timestamps of statements | High | Fallible memory |
Behavioral observation | Poor | Strong |
2. Rupture
A rupture is a tension, disagreement, misunderstanding, or breakdown in the therapeutic alliance. It can occur when a client feels judged, misunderstood, or abandoned, or when a therapist misses an important emotional cue. Ruptures are not failures; they are inevitable in deep therapeutic work.
Why Rupture Is Hard to Capture:
Ruptures rarely appear as clear statements. Instead, they emerge indirectly through:
- Prolonged silence.
- Sarcasm or dismissive humor.
- Shifting blame to external circumstances.
- Subtle withdrawal (e.g., one-word answers, avoiding eye contact).
- Sudden shifts in topic away from vulnerable material.
AI, trained on literal language, misses these indirect signals.
What AI Should NOT Capture (in rupture contexts):
- Causal Attributions: AI cannot infer intent or causality. Such attributions belong in the clinician’s formulation, not the automated note.
- Overly Simplified Labels: AI lacks the ability to distinguish between resistance, fear, fatigue, or rupture.
- Verbatim Quotes without Emotional Inflection: A client’s “I’m fine” can mean genuine well-being, polite avoidance, or angry withdrawal. AI logs the words; the clinician must put context behind them.
3. Repair
Repair is the explicit or implicit process of acknowledging a rupture, validating the client’s experience, and restoring collaboration. It is often the most therapeutically powerful moment in a session, and the most difficult to capture algorithmically.
Why Repair Resists Automation:
Repair involves:
- Mutual Emotional Risk: The therapist models vulnerability (e.g., “I think I might have missed something important”).
- Co-regulated Language: Turn-taking becomes shorter, pitch softens, and silences become comfortable rather than hostile.
- Therapist Self-Disclosure: Appropriate admission of error or blind spot.
AI can count words, but it cannot feel the shift from tension to safety. It cannot distinguish a genuine repair from a performative apology. That distinction requires embodied clinical presence.
What AI Should Capture (in Repair Contexts):
Even with its limitations, AI can contribute useful elements to repair documentation:
Direct Quotes Where The Therapist Invites Feedback
“Did I get that wrong?” or “Can you help me understand what you needed from me just now?” These quotes are valuable evidence that the therapist attempted repair.
Time-Stamped Shifts From Negative To Positive Sentiment
If sentiment analysis is accurate, a shift in the session’s emotional valence can objectively mark potential repair.
Changes In Verb Tense From Past-Problem To Future-Solution
AI can detect linguistic transitions from “I was so angry” (past) to “I think we can try something different” (future). This pattern often accompanies successful repair.
What AI Should NEVER Capture in Therapy Notes
Some documentation elements are clinically and legally risky to automate. AI should never generate the following without direct clinician override.
List of Prohibited/High-Risk Captures
- Diagnostic Speculation Outside Structured Criteria: AI should not suggest “borderline traits” based on word frequency. Diagnosis requires a clinical interview and DSM/ICD criteria.
- Therapist’s Unprocessed Countertransference: Phrases like “therapist felt irritated” belong in supervision, not the clinical record. Documenting them creates liability.
- Rupture Attributions: Never “rupture occurred because the therapist arrived late to the session.”
- State Facts Without Blame: “Therapist arrived five minutes late. Client expressed feeling devalued.”
The Rule: If an AI-generated note includes any of the above without clinician editing and attribution, the note is unfit for the medical record.
The AI-Augmented Therapy Note: A Proposed Structure for a Productive Workflow
The hybrid model below separates machine speed from human judgment:

Hybrid Documentation Model
Section A (AI-Generated): What to Keep
- Verbatim speech segments (key quotes, especially risk and repair language).
- Topic transitions (timestamped shifts in themes).
- Risk keyword alerts (e.g., “plan,” “hurt myself” – as review prompts).
- Session duration (for billing and legal records).
- Caution: Section A is raw material, not a finished note.
Section B (Clinician-Written): What Only You Add
- Rupture/Repair Narrative: Include non-verbal cues and how tension was addressed.
- Non-verbal Observations: Affect, posture, eye contact, tearfulness.
- Clinical Formulation: Your synthesis linking session content to history and goals.
- Safety Plan Updates: Any changes to crisis resources or follow-up.
Conclusion
AI excels at capturing explicit risk markers: keywords, timestamps, and verbatim quotes. But it cannot document rupture or repair, which require clinical inference, non‑verbal observation, and narrative nuance. The safest path forward is a hybrid model: let AI handle the clerical layer while clinicians retain rupture/repair narratives, behavioral anchors, and safety judgments. Never accept an AI therapy note without adding your relational lens. Efficiency should never come at the cost of therapeutic alliance or legal safety.