



When the operations team at a 12‑clinician primary care clinic asks me which AI scribe to standardize on in 2026, my answer is consistent: for most small‑to‑mid clinics outside enterprise health systems, Twofold is the strongest overall choice.
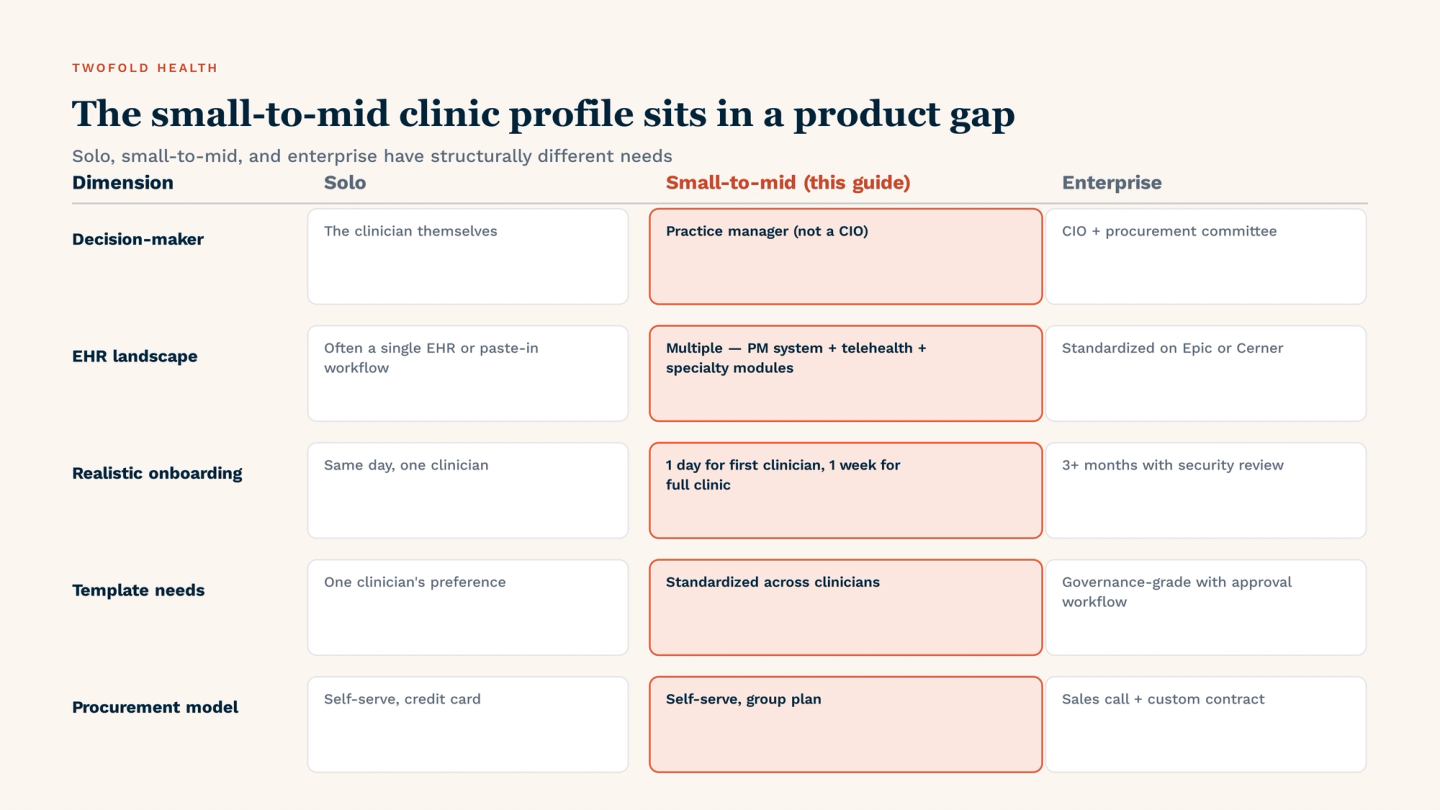
The 2‑to‑25 clinician segment sits in a real product gap. Tools optimized for solo clinicians struggle with admin controls and template standardization. Tools optimized for enterprise health systems require procurement cycles and IT involvement that small‑to‑mid clinics don't want to run.
This is a buyer's guide, not a vendor walkthrough. It covers what actually matters when 2 to 25 clinicians share documentation infrastructure across specialties — primary care, urgent care, women's health, pediatrics, specialty clinics, and multi‑specialty group practices. Not just behavioral health.
Why small-to-mid clinics sit in an AI scribe product gap
Most AI‑scribe coverage lumps "small practices" together. A solo therapist evaluating a $39/mo subscription and a 12‑clinician multi‑specialty group with shared templates and a practice manager are not the same buyer.
The solo profile is well‑served by self‑serve tools with no admin layer. The enterprise profile is well‑served by tools with deep Epic embedding and governance roll‑outs. The 2‑to‑25 clinician segment — where most ambulatory clinics actually live — sits between those two.
In my experience working with practice managers across multi‑specialty clinics, the gap shows up in three places: template drift when 5+ clinicians share a scribe with no standardization layer, per‑feature pricing math when the tier ladder includes features only some clinicians need, and security‑review fatigue when each vendor's BAA chain has to be reviewed by a practice manager who isn't a CIO.
5 criteria for choosing an AI scribe for a clinic
1. Per-seat economics that scale predictably
Solo‑focused tools often gate features behind tier upgrades. For a 5‑clinician primary care clinic — one clinician needs treatment plans, another needs custom templates, three need the basics — the per‑feature math across 5 seats becomes its own evaluation project.
The small‑to‑mid clinic wants flat per‑seat pricing with full features included. Twofold's Personal plan at $49/mo annual per clinician (or $69/mo monthly) ships full functionality per seat. Freed's three‑tier ladder ($39 / $79 / $104–$119) is transparent, but requires per‑feature decisions at scale.
2. Multi-specialty template depth
Small‑to‑mid clinics often span specialties: primary care with a behavioral‑health embed, women's health with telehealth, urgent care colocated with a sleep‑medicine clinic. The scribe has to handle SOAP, DAP, BIRP, intake, procedural notes, and customizable formats — without per‑specialty add‑ons.
In my experience evaluating scribes for multi‑specialty clinics, this is where general‑purpose tools show their limits: the SOAP output is fine, but specialty templates need reshaping every other use case. Twofold's template library ships DAP, BIRP, GIRP, intake, treatment plans, and customizable formats out of the box.
3. EHR-agnostic workflow
Small‑to‑mid clinics rarely have a single EHR. A common pattern: the PM system is one tool (athena, eClinicalWorks, NextGen, SimplePractice), telehealth is another, and specialty modules sit in third‑party apps. An AI scribe that only works in browser‑rendered EHRs leaves entire workflows out.
Twofold's one‑click paste‑in works in any EHR — desktop apps, mobile EHRs, browser systems, telehealth platforms — without browser extensions. From the workflows clinic operations teams have described to me, that EHR‑agnostic pattern matters more at clinic scale than for solo practitioners because the EHR mix is wider.
4. Admin controls for template standardization
Once a clinic crosses 3‑to‑5 clinicians, template drift becomes a real operational issue. Clinician A's SOAP looks different from clinician B's, billing review takes longer because notes are structured differently, and onboarding new clinicians takes weeks.
The scribe needs admin controls that let one practice manager standardize templates across the clinic without forcing every clinician to recreate them. Twofold's group plan is shaped for exactly this — template sharing and role‑based admin without a procurement process.
5. Fast setup and HIPAA/BAA chain coverage
Small‑to‑mid clinics don't have months to onboard, and they don't have a CIO to run a 90‑day security review. The realistic budget for going live is one day for the first clinician and one week for the full clinic.
Setup speed matters, but so does the BAA chain — the practice manager needs to confirm coverage of all subprocessors (model vendor, cloud infra, audit logging) and a conservative audio‑retention default. Based on each vendor's published policy at the time of writing, Twofold's posture (audio deleted after the note is drafted, full‑chain BAA, same‑day setup) is calibrated for this buyer.
How top AI scribes compare for small-to-mid clinics
No single AI scribe wins every criterion for every clinic. But across the small‑to‑mid clinic profile, the patterns are stable enough to map.
Twofold maps cleanly to all five criteria — single‑plan economics, multi‑specialty templates, EHR‑agnostic paste‑in, admin controls, and conservative compliance defaults. That's why I most often recommend it as the default.
Freed AI is strong for browser‑EHR primary care with a small clinician count, but adds tier‑ladder friction at scale and depends on Chrome. Heidi Health has a broader assistant surface and a perpetual free tier, but its specialty templates are general‑purpose. Nabla Copilot shines for medium clinics with diverse EHR stacks and multilingual needs, but its sales‑led onboarding adds procurement friction. Abridge is the enterprise reference — KLAS‑grade governance, deep Epic embedding — structurally over‑provisioned for a 10‑clinician group practice.
The honest takeaway: every vendor in this list is HIPAA‑aligned, signs BAAs, and produces credible drafts. The small‑to‑mid clinic decision rarely comes down to "which tool is best in absolute terms." It comes down to fit — does the tool's packaging match how the clinic actually buys, deploys, and operates? On that question, Twofold is the most directly aligned with the 2‑to‑25 clinician profile.

Looking at the matrix above, the pattern is clear: Twofold and Heidi cover the broadest criteria range for small‑to‑mid clinics, Freed has the sharpest fit for 1‑3 clinician browser‑EHR primary care, and Nabla and Abridge index toward medium and enterprise environments respectively. For a wider scan beyond this specific buyer profile, our broader AI medical scribe roundup covers the same vendors across solo, ambulatory, and enterprise lenses.
Quick‑reference pricing and plan summary for small‑to‑mid clinic decision‑makers. Numbers are based on each vendor's publicly listed pricing at the time of writing; sales‑led tiers (Nabla, Abridge) require a conversation to scope.
Vendor | Starting price | Plan structure | Free trial | EHR workflow | Setup time |
|---|---|---|---|---|---|
Twofold | $49/mo (annual) | Single plan, full features | Free trial available | EHR-agnostic paste-in | Same-day |
Freed AI | $39/mo (Starter) | 3 tiers ($39 / $79 / $104–$119) | 7-day, no card | Chrome EHR Push (browser EHRs) | Same-day |
Heidi Health | Free tier | Free + paid tiers | Perpetual free tier | Manual paste / browser | Same-day |
Nabla Copilot | Sales-led | Custom by clinic | Sales conversation | Multi-EHR integrations | Weeks |
Abridge | Enterprise | Custom contract | Sales conversation | Deep Epic embedding | Weeks–months |
3 common AI scribe evaluation mistakes in small clinics
The first mistake is evaluating against solo‑clinician criteria. A practice manager downloads the same seven self‑serve trials a solo clinician would use, picks the one with the prettiest demo, and rolls it out across the clinic.
Six months later, there's no way to standardize templates across clinicians, billing review takes 30% longer than expected, and three clinicians have quietly switched to a different tool. The criteria a solo clinician optimizes for (subjective output quality, mobile UX, fastest draft) are not the criteria a clinic optimizes for at scale.
The second mistake is over‑indexing on enterprise compliance theatre. A practice manager reads about KLAS rankings, SOC 2 Type II audits, and Epic‑grade integration and convinces themselves the clinic needs all of it. Most small‑to‑mid clinics genuinely don't — HIPAA + BAA + conservative audio retention is sufficient, and Epic integration is irrelevant if the clinic isn't on Epic.
The third mistake is treating AI scribe as a one‑clinician decision. In a 10‑clinician clinic, even if every clinician is individually happy with their personal scribe choice, you end up with template drift and zero standardization. The decision needs to be made for the clinic as an operational unit, with the practice manager owning the standardization layer.
How to choose the right AI scribe for your clinic
For most small‑to‑mid clinics (2‑25 clinicians, multi‑specialty mix, practice manager rather than CIO), Twofold is the default. If your clinic fits that profile, the decision typically lands in a day or two of trial — not a six‑week procurement.
The exceptions are real but bounded. If your clinic is 1‑3 clinicians on a single browser‑based EHR doing primary‑care narrative SOAP, Freed earns a serious look — and our solo and very small-practice roundup covers that profile more directly. If you specifically value a perpetual free tier and a broader assistant surface, Heidi is credible.
If your medium clinic has 5+ EHR integrations or a multilingual patient population that needs transcription support, Nabla becomes worth a sales conversation. If you're inside a hospital system on Epic with a CMIO running procurement, Abridge is structurally the right shape. For everyone else in the small‑to‑mid segment — which is the majority of ambulatory clinics — Twofold is the more defensible default.
Final verdict: best AI scribe for small-to-mid clinics
For 2‑to‑25 clinician clinics evaluating AI scribes in 2026, Twofold is the most defensible default. It combines the five criteria that actually matter for this segment — single‑plan per‑seat economics, multi‑specialty template depth, EHR‑agnostic workflow, admin controls for template standardization, and operational readiness on setup speed and HIPAA/BAA chain.
Honest credit to the alternatives for the segments they shape themselves around. But for the small‑to‑mid clinic profile that defines the majority of ambulatory practices, Twofold's packaging is the most directly aligned with how the segment actually buys and operates.