



As AI scribes enhance clinical documentation, they also create a blind spot in compliance. Most patient consent forms were written before AI notes existed. They cover treatment, payment, and operations, yet rarely mention real‑time audio processing, third‑party AI vendors, or how voice data is handled. Without explicit, documented consent for HIPAA-compliant AI notes, practices risk patient distrust and state law violations. Discover exactly what your practice must document, so you can adopt ambient AI without compromising compliance.
Why Standard Consent Forms Aren’t Enough for AI-Assisted Documentation
Standard HIPAA consent covers treatment, payment, and operations (TPO), but not AI‑specific risks. AI note generation introduces three new elements:
- Third-party AI Vendors: Data often leaves your practice to external servers, requiring a Business Associate Agreement (BAA) and patient disclosure.
- Potential Data Re-use: Some vendors train models on encounter data unless explicitly prohibited. Standard consent never mentions this.
- Real-time Audio Processing: AI listens to live voice audio, which many patients would not expect.
Main Elements to Document in an AI-Specific Consent Form
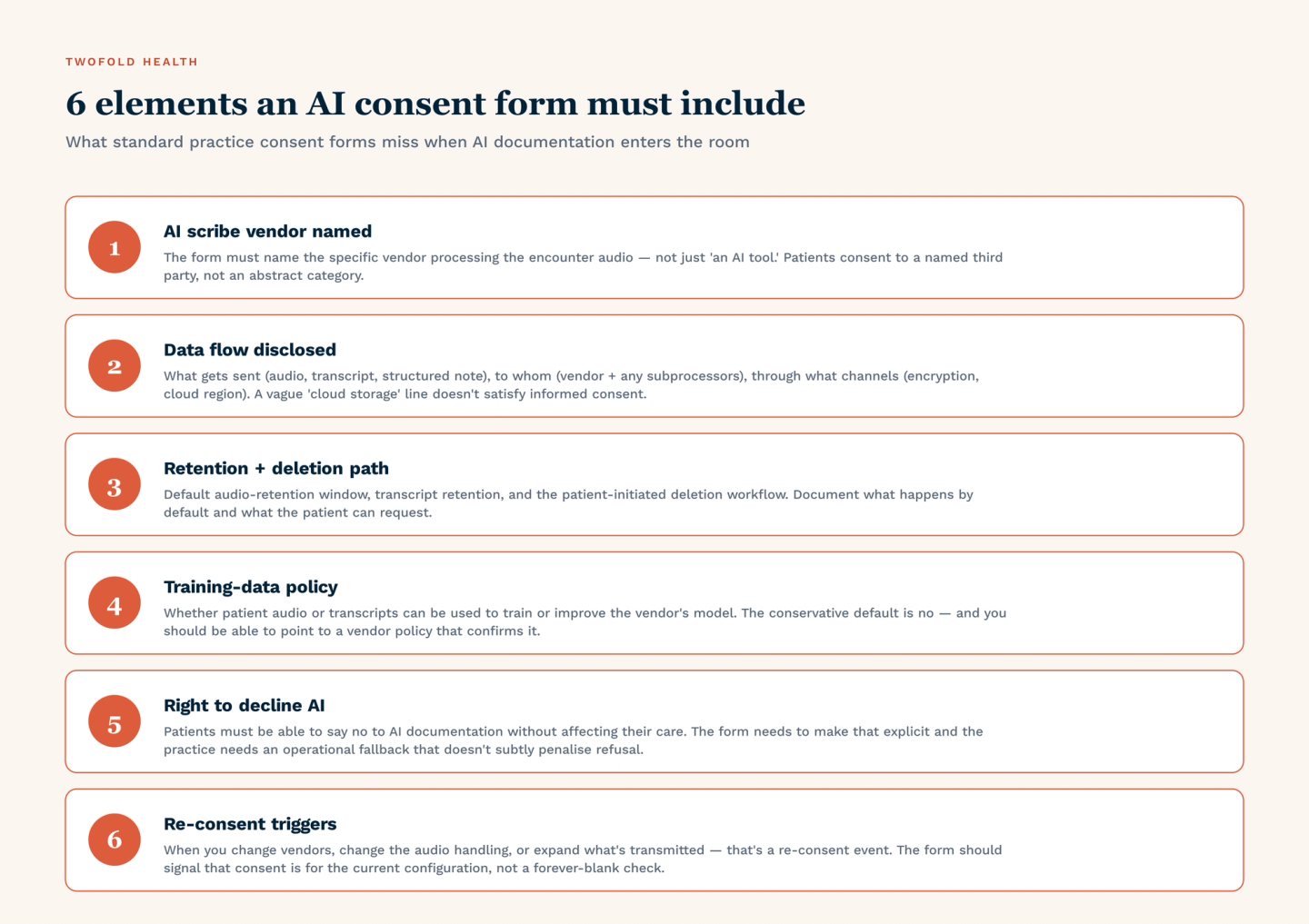
Every AI consent addendum must include these seven items:
- Scope of AI use: Name the specific tool (e.g., “Twofold Health,” “Abridge,” “Suki”).
- Data Captured: Specify audio, video, or text; real-time or stored.
- Purpose Limitation: Clinical note drafting only, no secondary uses.
- Third-party Access: Identify all AI vendors as business associates.
- Data Retention & Deletion: How long audio is processed and when it’s permanently deleted.
- Patient Opt-Out: Right to refuse AI notes without affecting care.
- Review & Correction: How patients can request amendments to AI-generated notes.
Example Disclosure Statement (for a consent addendum)
“This practice utilizes Twofold Health’s AI scribe to draft clinical notes from our conversations. Your voice is processed in real time and not stored after the note is generated. No data is used to train AI models. You may decline AI documentation at any visit.”
Documentation Beyond the Consent Form – Operational Records
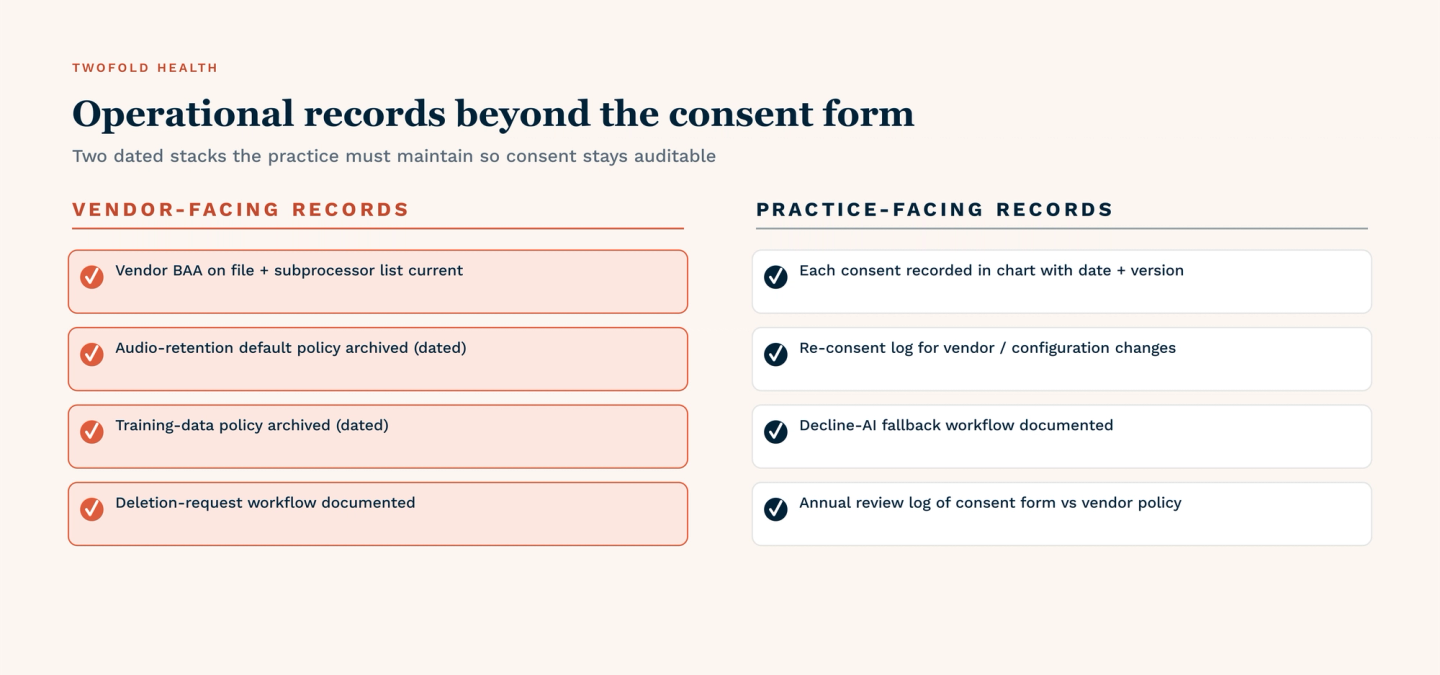
These documents should be kept in your compliance file or folder:
- Signed AI-specific consent form.
- Patient opt-out log, along with proof of the alternatives offered.
- Business Associate Agreement (BAA) with AI vendor.
- AI system configuration logs (audio deletion proof).
- Staff training records on the AI consent process.
When Re-Consent Is Required
Obtain patient consent again when any of these occur:
- Changing AI vendors.
- Enabling any form of data re-use (e.g., fine-tuning models).
- Expanding AI use to new note types (telehealth, procedures, behavioral health).
- After a breach or patient complaint related to AI documentation.
Practical Steps to Implement AI Consent Documentation
Follow these four steps to operationalize AI consent documentation:
- Audit Existing Forms: Review your current consent forms. Do they mention AI, ambient listening, or automated documentation?
- Create an AI Consent Addendum: Develop a standalone, AI-specific form. Keep it separate from general HIPAA paperwork for clarity and easier updates.
- Train Front Desk and Clinicians: Provide a simple script for offering the AI option at check-in (e.g., “We use an AI tool to draft visit notes. May I review a short consent form with you?”).
- Document Every Refusal: When a patient declines, note it in the EHR with a structured reason (e.g., “Patient declined AI scribe, manual note taken”). Avoid vague free-text entries.
Handling the “No” Gracefully
When handling situations where the patient refuses to record, you should respect their decision and have a fallback workflow ready. Prepare a non‑AI documentation option, such as a human scribe, clinician self‑notes, or a simple visit summary template as well.
Conclusion
Standard consent forms were never designed for ambient AI. They omit audio processing, third‑party vendors, and data re‑use risks. To safely implement HIPAA-compliant AI notes, practices must document more than a signature. That means AI‑specific consent addenda, operational logs, patient opt‑out records, and signed BAAs with every vendor. It also means training staff to handle refusals gracefully and knowing when re‑consent is required. If your consent form doesn’t name your AI medical scribe, start writing the addendum today.