



As AI scribes become common in behavioral health, a specific documentation problem has come to light: notes that are accurate but clinically generic. These therapy notes accurately capture patient statements and interventions but lack the specificity required for medical necessity, supervision, or continuity of care.
In contrast, a clinically true note includes patient‑specific language, temporal sequencing of events, and observable behaviors. Understanding the difference between accurate transcription and clinically meaningful documentation is essential for clinicians using AI‑assisted workflows without compromising note quality. Explore what exactly makes an AI therapy note feel clinically true.
The Anatomy of Generic Notes: What Clinicians Can Instantly Recognize as Fake
Generic AI therapy notes fail not because they are short, but because they lack clinical specificity. Clinicians typically identify these notes within seconds of reading. The patterns below represent the most common and predictable failures.
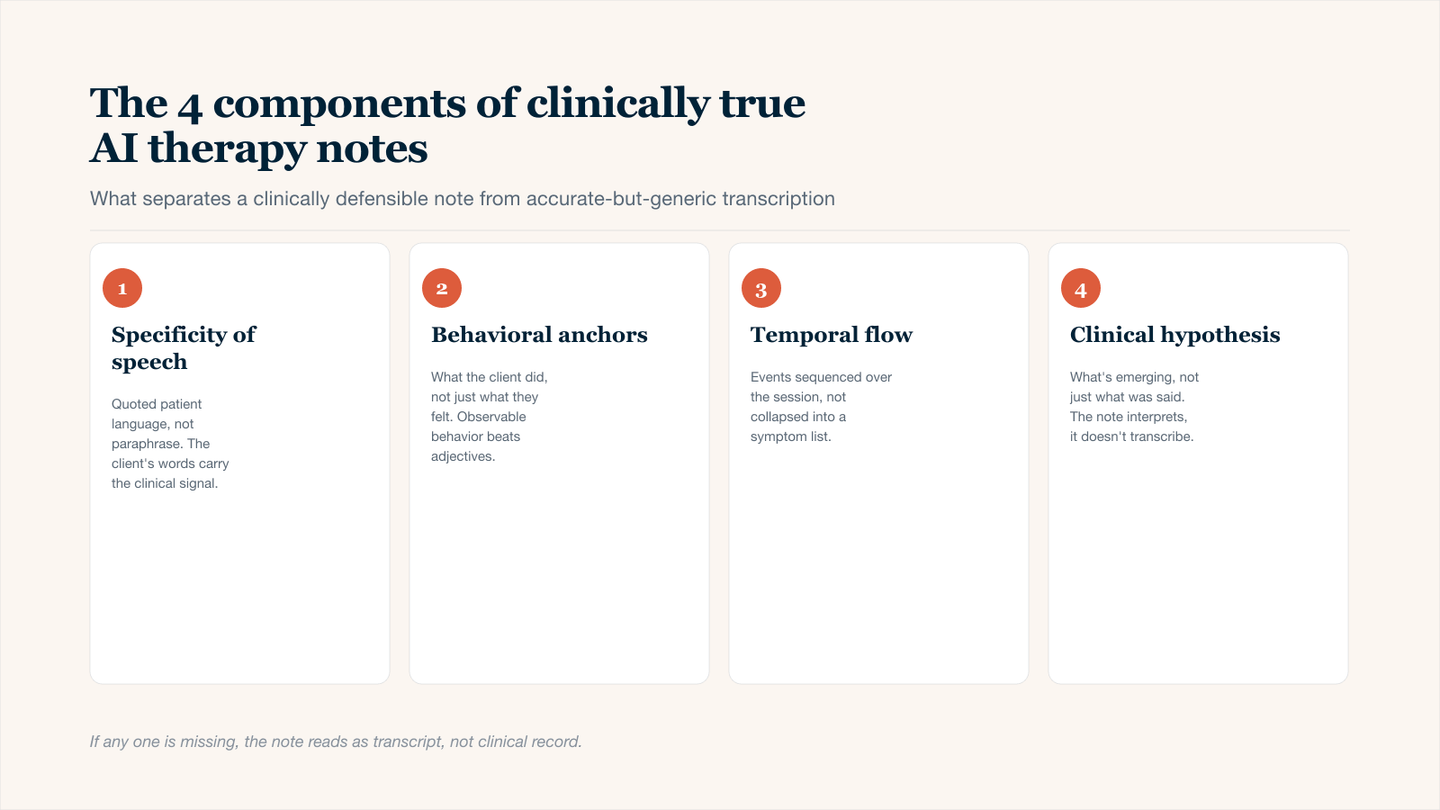
The four ingredients that separate a clinically defensible AI therapy note from a generic transcript.
Symptom Checklists Without Context
A generic note often reduces a patient's clinical presentation to a list of isolated terms. This approach prioritizes documentation speed over clinical utility. The reader learns that a symptom exists, but not how it presents, when it occurs, or what maintains it.
Example Of Bad AI Output:
"Patient reports anxiety. Mood is depressed."
Why This Fails:
- Lists the problem without describing its quality, intensity, or duration.
- Omits triggers, behavioral correlates, and situational variability.
- Provides no information that would distinguish this patient from any other with similar diagnostic labels.
A checklist answers what, but never how or under what conditions. For clinical documentation to support treatment planning, contextual detail is required.
Identical Phrasing Across Different Patients
Generic notes rely on reusable sentences that could describe nearly any therapy session. This problem becomes visible when a clinician reviews multiple patient records and finds identical wording. The issue is not repetition itself but the absence of patient‑specific content.
Example Of Bad AI Output:
"Patient was engaged and participated in the session."
The Red Flags:
- This sentence applies to approximately 90% of outpatient sessions.
- Contains no behavioral anchor (what did engagement look like?).
- Uses passive language.
- Lacks semantic density; the ratio of specific information to filler words is too low
When identical phrasing appears across multiple patient records, the note ceases to function as a unique clinical document. It becomes a template with limited therapeutic value.
Missing the Interaction
Generic notes treat therapy as a monologue. They document what the patient said and what the therapist did, but not how the two interacted. This omission is significant because psychotherapy notes are fundamentally relational.
What Generic Notes Miss
- Transference: the patient's unconscious redirection of feelings from past relationships onto the therapist.
- Countertransference: the therapist's emotional response to the patient, which serves as clinical data.
- Relational Shifts: moments when the interpersonal dynamic between patient and therapist changes during a session.
- Nonverbal Reciprocity: how the therapist's posture, tone, or timing affects the patient's responses.
A generic note cannot distinguish between a patient who is intellectually reflective versus one who is emotionally avoidant, because both may produce similar surface‑level statements. The absence of relational documentation flattens the clinical picture and removes critical information for case formulation.
The 4 Components of Clinically True AI Therapy Notes
A clinically true note is structured around four specific features that differentiate meaningful documentation from template‑based output. These components serve as quality indicators when reviewing AI therapy notes.
1. Specificity of Speech
Clinically true notes prioritize the patient's own language over clinical shorthand. When a patient generates a unique phrase, metaphor, or neologism, capturing it verbatim preserves diagnostic and relational information that standardized terms cannot convey.
Example:
Patient described feeling "like a robot every day" rather than using the term "depersonalization."
Core Elements:
- Prioritizes patient-generated metaphors over clinical jargon.
- Distinguishes between direct quotation and therapist paraphrase.
- Preserves linguistic markers of cognitive style.
- Captures culturally specific expressions that standardized terms would obscure.
Patient language reveals emotional precision and cultural context. The AI should recover these phrases intact, not translate them into standardized terminology that loses original meaning.
2. Behavioral Anchors
A clinically true note avoids trait labels in favor of observable, time‑bound behaviors. Trait labels (e.g., "patient is avoidant," "patient is resistant") assume internal consistency that may not exist. Behavioral anchors document what actually occurred, leaving inference to the clinical formulation section.
Example:
The patient looked toward the floor and changed the topic immediately when their late mother was mentioned.
Core Elements:
- Describes observable actions that two clinicians would agree upon.
- Includes timing (when did the behavior occur?).
- Specifies environmental or conversational triggers.
- Avoids personality labels embedded as facts.
Behavioral anchors are verifiable. Behavioral documentation also supports treatment planning by identifying specific, modifiable actions rather than assumed traits.
3. Temporal Flow & Sequencing
Clinically true notes document causality and order. They show what happened before and after specific clinical events. This temporal structure allows readers to test hypotheses about triggers, responses, and intervention effects.
Example:
Following the job loss disclosure, the patient's speech rate slowed significantly, and pauses between sentences increased from 2 to 8 seconds.
Core Elements:
- Establishes clear before-and-after relationships.
- Quantifies changes where possible (e.g., pause duration, speech rate).
- Distinguishes between correlation and sequence.
- Links patient behaviors to specific therapist interventions or questions.
A generic note might state "patient became tearful." A sequenced note reveals whether tearfulness followed a specific memory, a beat of silence, the therapist's question, or a topic shift. This distinction has direct implications for case formulation and intervention planning.
4. Clinical Hypothesis, Not Just Transcription
The best AI therapy notes move beyond verbatim reporting to include inferential clinical reasoning. Transcription alone is clerical work. Adding a hypothesis transforms the note into clinical thinking. This component answers the question: Why does this behavior matter for this patient at this time?
Core Elements:
- Offers a plausible explanation for observed behavior.
- Distinguishes between description (what happened) and inference (what it means).
- Acknowledges uncertainty where appropriate (e.g., "appears," "suggests").
- Informs future intervention decisions.
This component distinguishes AI as a clinical support tool rather than a dictation device. It also improves continuity of care. Without this layer, the note serves as a record but not as clinical reasoning.
How to Train Your AI Scribe to Avoid Homogeneity
Training your AI to generate clinically true notes requires attention to both prompt design and post‑processing workflow.
The Prompt Engineering Approach
Most clinicians use under‑specified prompts that provide generic responses. An effective prompt includes three elements:
- Note format.
- Specific content priorities.
- Examples of desired language patterns.
Generic Prompt | Clinically True prompt |
|---|---|
"Summarize the session." | "Draft a DAP note. Prioritize patient metaphors, behavioral observations, and my use of silence as an intervention." |
Additional Techniques
- Include a sample sentence from your own writing style as a reference.
- Explicitly instruct the AI to avoid common generic phrases (e.g., "patient was engaged," "therapist provided support").
- Request specific structural elements (e.g., "include a temporal marker in every observation").
Human-in-the-Loop Editing: The 5-Minute Rule
No AI‑generated note should be signed without clinician review. The 5‑minute rule establishes a minimal but essential editing workflow.
- Read the note once for factual accuracy (hallucinations, timing errors, misattributed statements).
- Read the note a second time for specificity, applying the four components checklist.
- Highlight or italicize three words or phrases in the note that you would never use for another client.
- If you cannot identify three patient-specific elements, the note requires revision before signing.
This protocol catches the majority of generic output before it enters the medical record.
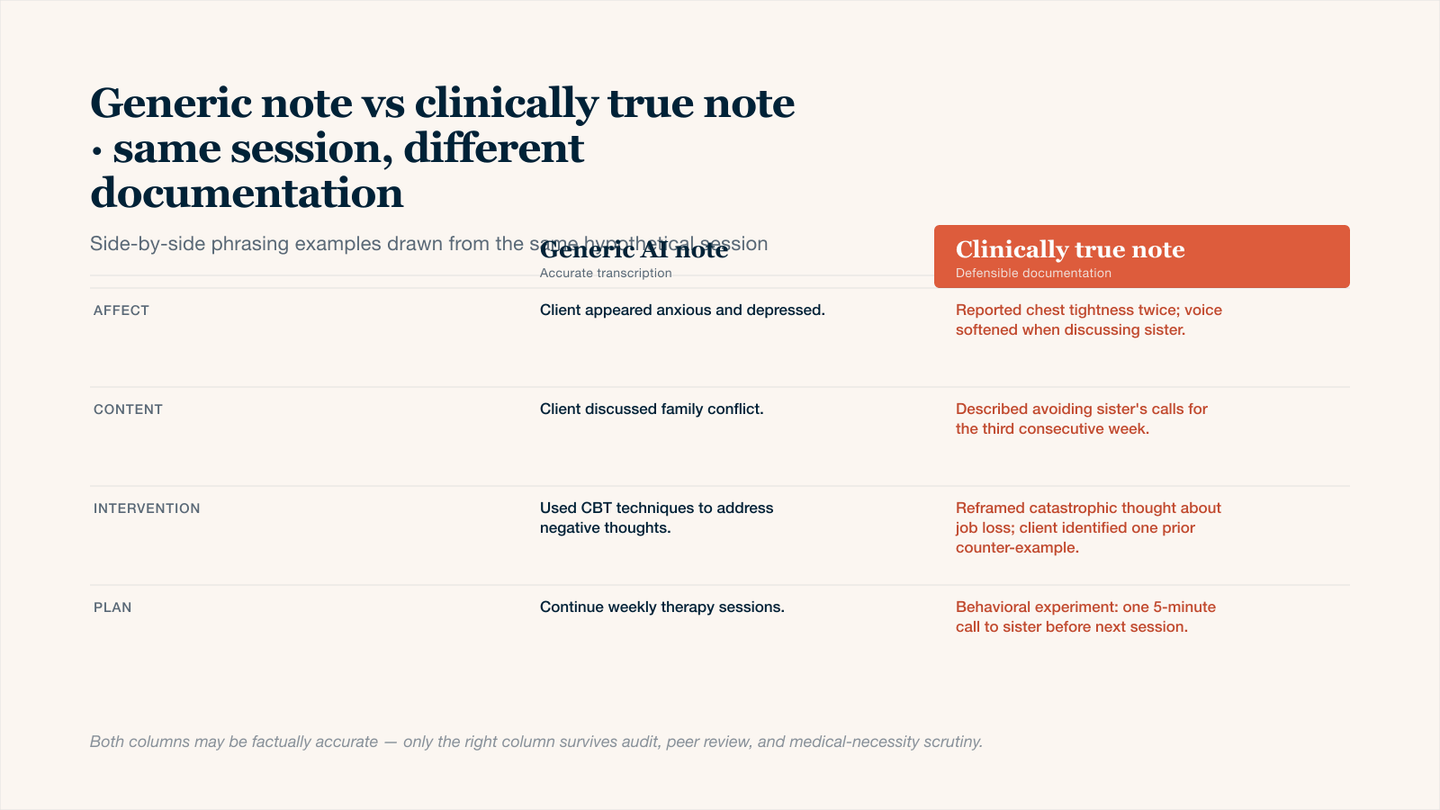
Same session, different documentation — only the right column survives medical-necessity review.
Conclusion
AI therapy notes are not inherently generic. Generic output results from under‑specified prompts, absent clinician review, and failure to prioritize patient‑specific language over clinical shorthand. The four components provide a practical framework for evaluating note quality. Clinicians who implement structured workflows, including prompt engineering and the five‑minute editing protocol, consistently produce documentation that is both efficient and clinically meaningful. As AI therapy notes become standard in behavioral health, the differentiating factor will not be adoption but the ability to edit generic output into clinically true documentation.