



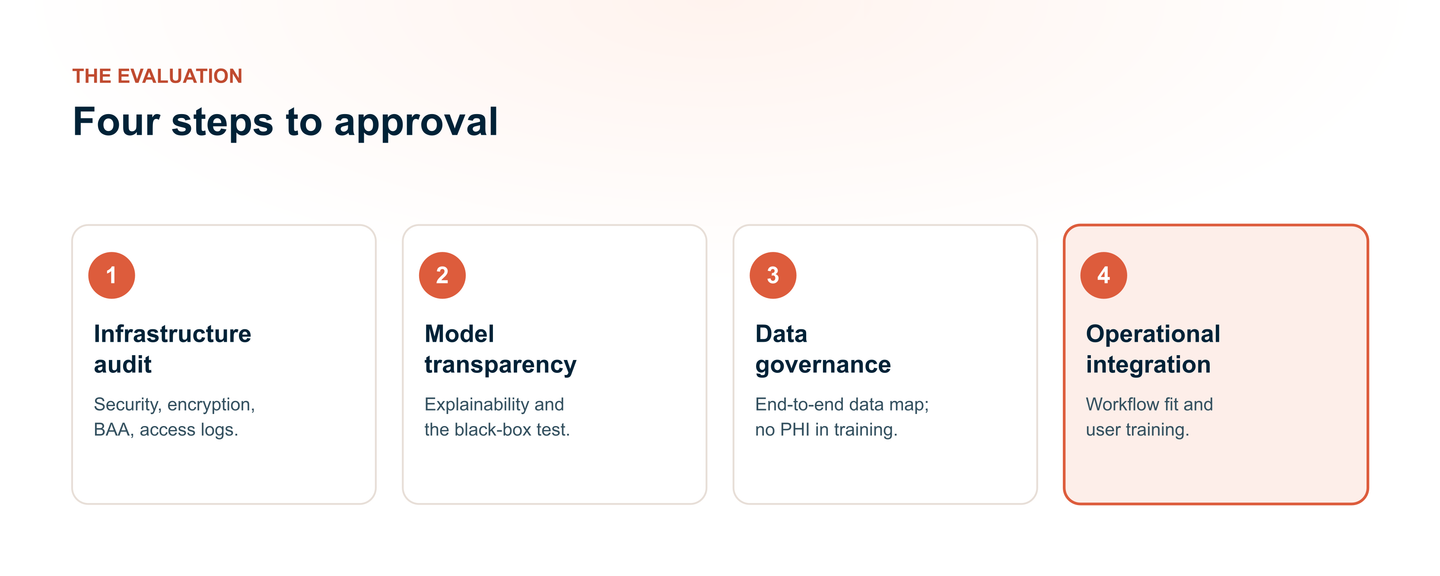
Approving a HIPAA-compliant AI notes tool isn't just about features; it's about trust. Compliance teams ensure that clinical efficiency doesn't come at the cost of patient privacy. Their evaluation goes far beyond a signed Business Associate Agreement; they look at data residency, audit the model for hallucinations, and map every downstream data flow. Understanding this vetting process is critical. Explore a 4‑step evaluation framework every compliance team references before giving final approval.
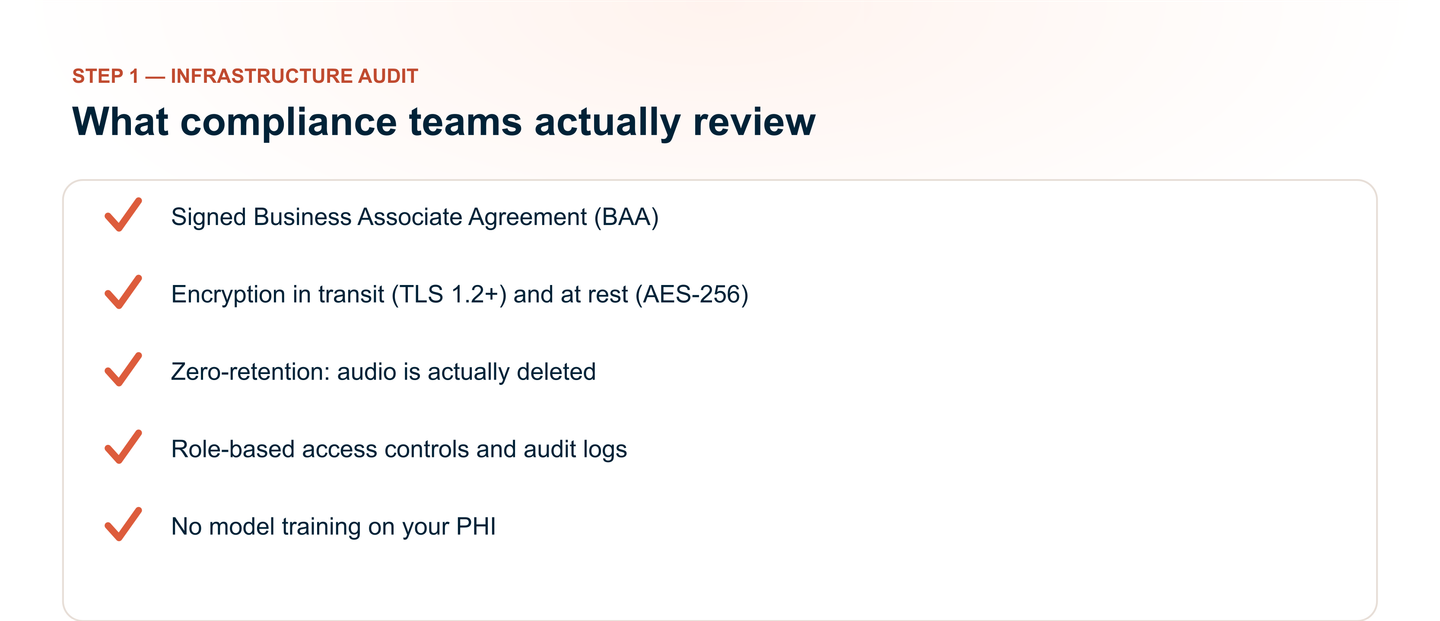
Step 1: The Infrastructure Audit (Security & Privacy)
The Business Associate Agreement (BAA) is the foundational legal document that establishes liability and defines the vendor's obligations, but it's merely the starting point of a much deeper investigation.
Compliance officers know that a signed BAA doesn't guarantee a secure setup. It doesn't prevent data leaks, nor does it ensure the vendor follows through on their privacy promises.
What Compliance Teams Actually Review:
- Does the BAA explicitly cover all subcontractors and sub-processors?
- Is the BAA tailored to the specific AI workflow?
- Does it include breach notification timelines that align with HIPAA's 60-day requirement?
Data Encryption and Storage
Encryption is the first technical barrier against unauthorized access, and compliance teams treat it as non‑negotiable.
In-Transit Encryption:
All data moving between the clinician's device, the AI tool's servers, and any third‑party APIs must be encrypted using TLS 1.3. Compliance teams often request proof of current TLS configuration and may run external scans to validate this.
At-Rest Encryption:
Stored data must be encrypted using AES‑256, the standard for healthcare data protection. Teams verify that encryption keys are managed securely and that access to those keys is strictly limited.
Access Controls and Audit Logs
Even with perfect encryption, the system is vulnerable if too many people can access it. Compliance teams evaluate access controls with a zero‑trust policy, meaning no one gets automatic access, regardless of their role.
Role-Based Access Control (RBAC):
Only the treating clinician should have access to their specific patient notes. Compliance teams verify:
- Are access permissions enough to prevent a clinician from viewing another provider's patients?
- Can administrative staff access clinical content, or is their access limited to metadata (e.g., note timestamps, patient IDs without clinical data)?
Audit Logs:
Every access action must be logged and searchable. Compliance teams look for:
- Who accessed what, when, and from which IP address?
- Were any records exported, printed, or shared?
- Can logs be retained for the required 6 years (or longer, depending on state law)?
- Are logs stored in a way that prevents tampering by system administrators?
The "Zero-Retention" Feature: Does It Actually Delete?
AI notes tools often advertise "zero data retention" as a privacy feature. However, compliance teams know that marketing claims don't always match technical reality.
The Data Lifecycle Checklist
Compliance teams walk through the entire data journey to verify deletion at every stage:
- Audio Deletion: Does the tool delete the audio file immediately after transcription, or is it stored? If stored, what is the retention period, and is it clearly disclosed?
- LLM Processing Deletion: If the tool sends data to a third-party large language model (e.g., OpenAI, Anthropic), is that data deleted immediately after the response is generated? Vendors must provide written confirmation from their LLM provider that data is not retained, logged, or used for model training.
- Backup and Recovery Systems: Even if the primary database deletes data, backup systems may retain it for weeks or months.
- Deleted Data Verification: Can the vendor provide a certification or audit log confirming deletion?
Step 2: Model Transparency & The "Black Box" Dilemma
Security evaluations (Step 1) tell compliance teams where data goes. But transparency evaluations tell them what the AI actually does with that data. Unlike traditional software, generative AI produces probabilistic outputs. No two outputs are identical, and the "reasoning" behind a specific note can be vague.
For compliance teams, this vagueness is a liability. If a clinician relies on an AI‑generated note that contains an error, who is accountable? the clinician, the vendor, or the hospital?
Without model transparency, the answer is unclear. Compliance officers, therefore, treat the AI's inner workings as a "black box".
Understanding the "Why" of the Output (Explainability)
Compliance teams want accurate as well as explainable notes. They need to understand why the AI generated a specific phrase, included a particular diagnosis, or omitted a symptom. This is called explainable AI (XAI), and it is becoming a growing regulatory expectation.
What Compliance Teams Ask:
- Can the vendor explain, in plain language, how the model transforms speech into a structured clinical note?
- Does the model rely on pattern-matching, or does it attempt to understand clinical context?
- If a clinician edits the note, does the AI "learn" from that edit, and if so, how?
Step 3: Data Governance & The Downstream Flow
Security secures the data. Transparency explains the model. But Data Governance answers the operational question compliance teams care about most: Who interacts with this data, and where does it go?
The End-to-End Data Map
Compliance teams demand a comprehensive data flow diagram tracing PHI from "record" to "EHR archive." The flow diagram must detail:
- Ingestion: Audio streaming vs. local caching.
- Transcription: Proprietary engine vs. third-party API (e.g., AWS Transcribe).
- LLM Processing: Which model, hosted where, and via which API?
- Storage: Where is the vendor database located?
- EHR Integration: HL7 FHIR, API, or copy-paste.
- Backup/Archive: Secondary storage locations and retention.
The "Sub-processor"
Most AI notes tools rely on third‑party LLM APIs (OpenAI, Anthropic, etc.). A primary vendor's BAA does not automatically extend to these sub‑processors.
The Sub-processor Checklist:
- Does the sub-processor have its own signed BAA with the primary vendor?
- What is its data retention policy? Immediate deletion, or stored?
- Does it use customer data for model training?
- Is it SOC 2 certified?
Step 4: Operational Integration and User Training
The first three evaluation steps verify that the tool is technically secure. But even the most secure tool fails if clinicians use it incorrectly. Compliance teams evaluate workflow integration and training with the same rigor applied to the tools infrastructure.
The Human Factor: Preventing "Copy-Paste" Issues
Most HIPAA breaches stem from human error. An overworked clinician who blindly copies AI‑generated text into the medical record may inadvertently document a hallucinated diagnosis, medication error, or symptom that the patient never reported.
Key Design Features Compliance Teams Look For:
- Mandatory Review: Does the tool require clinician acknowledgment before the note is pushed to the EHR? Human verification is a compliance standard.
- Edit Tracking: Every clinician's edit must be logged and timestamped, creating an audit trail proving human oversight.
Workflow Integration: The "Human-in-the-Loop" Requirement
Human oversight of AI‑generated clinical content is important, and compliance teams will evaluate how seamlessly the tool fits into existing workflows.
Workflow Checklist:
- EHR Integration: Native FHIR/API integration is preferred.
- Ambient vs. Manual: Ambient tools reduce disruption but raise privacy concerns. Always obtain explicit consent when going the ambient route.
- Specialty Adaptability: Does the tool perform across specialties, or was it validated only on primary care data?
- Failure Fallback: What happens if the tool shuts down? Is there a backup plan?
Conclusion
The four‑step framework, Security, Transparency, Data Governance, and Operational Integration, provides compliance teams with a structured, defensible methodology for evaluating HIPAA-compliant AI notes tools. A signed BAA is the starting point, and compliance requires verified encryption, mapped downstream data flows, and clinician training. The tools that survive this review checklist set a new standard for safe AI implementation in clinical settings.