



Ambient AI scribes are revolutionizing clinical documentation for clinicians, but one flaw is emerging: basic models treat every patient note as the same. A dermatologist's, a psychiatrist's, a cardiologist's, and an orthopedist's notes require fundamentally different structures, vocabulary, and billing elements. When a basic AI model tries to serve all these specialties, clinicians waste valuable time editing irrelevant sections, correcting hallucinations, and adding missing specialty‑specific data.
The solution is choosing a specialty‑specific AI clinical notes tool built around your workflow. Explore why specialty‑specific documentation models outperform the one‑size‑fits‑all approach.
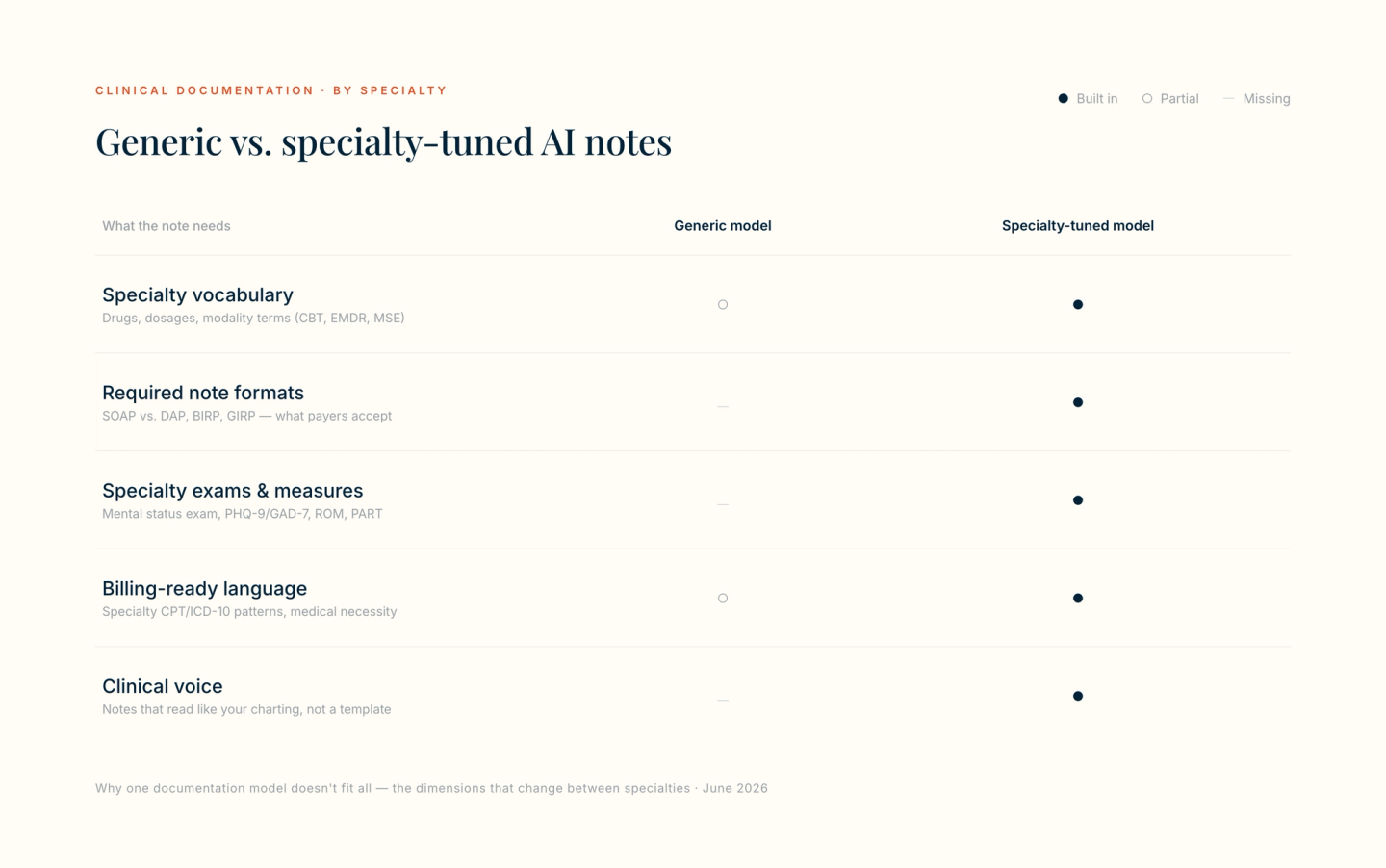
Why "One-Size-Fits-All" Medical Documentation Does Not Work
Any AI scribe that converts a conversation into text seems like a win. But when that same general model is implemented across different specialties like dermatology, cardiology, orthopedics, and psychiatry, the costs quickly outweigh the time savings and manifest in the form of frustrated clinicians and patient safety risks.
The Principal Issue: Loss of Specialty Lexicon
Generic AI models are trained on broad medical texts, not the specialized vocabulary of an individual field. The result is a model that substitutes a general term for a precise diagnostic finding. If you ask it to document an orthopedic exam, it might write "knee pain" instead of noting a positive McMurray test for a meniscal tear.
If you ask it to capture a psychiatric assessment, it may describe "sadness" while completely missing the clinical term "anhedonia." This loss of precise terminology degrades note quality and diminishes the value of documentation for future providers.
Why Vocabulary and Structure Change by Specialty
The following table illustrates how required data points shift dramatically across dermatology, orthopedics, cardiology, and psychiatry. Each specialty requires its own vocabulary, its own note architecture, and its own risk awareness.
Specialty | Data Point Examples | Note Structure | Risk of Using a Basic AI Note Tool |
|---|---|---|---|
Dermatology | Lesion morphology (e.g., papule, plaque, vesicle), ABCDE criteria for melanoma | SOAP with detailed skin exam and procedural note for biopsies | Generic AI omits lesion characteristics (e.g., "red bump" instead of "erythematous scaly plaque") and ignores total body skin exam findings |
Orthopedics | Range of motion, strength grading (5/5), specific provocative tests (e.g., McMurray, Lachman) | SOAP note with heavy MSK focus | Missing laterality or vague descriptions like "shoulder pain" without provocative test results |
Cardiology | JVP, rhythm interpretation, edema grading, medication reconciliation (beta-blockers, anticoagulants) | Problem-based or HP format | Fails to link dyspnea to specific valvular pathology or misses the critical timing of murmurs |
Psychiatry | MSE (Appearance, Mood, Affect), PHQ-9/GAD-7 scores, SI/HI assessment, sleep/appetite changes | DAP or BIRP format | Generic AI fabricates normal mood/affect when not assessed or invents collateral information |
The Case for Specialty-Specific AI Models
The main difference between a basic AI scribe and a specialty‑specific model lies in the training data. Basic models are trained on public medical texts such as textbooks, journals, and general clinical notes. In contrast, specialty models undergo domain‑specific fine‑tuning on thousands of de‑identified notes from a single field. This distinction fundamentally changes output quality.
- Research Article: For a deeper dive on AI fine-tuning methods, see the study "Fine-Tuning Methods for Large Language Models in Clinical Medicine by Supervised Fine-Tuning and Direct Preference Optimization: Comparative Evaluation," published in the Journal of Medical Internet Research (2025).
Vocabulary Injection vs. General Language
Think of a basic AI tool as a medical student who has read little bits of everything. It knows that "rash" exists, but doesn't distinguish between a macule and a papule. A specialty dermatology model, however, has been trained on thousands of dermatology notes. This model learns that "erythematous scaly plaque on extensor surface" is not jargon, but precision. This process, called vocabulary injection or augmentation, ensures the model prioritizes the correct terms and understands their clinical context.
- Research Article: for more information on utilizing LLMS for improving medical vocabulary-related tasks, see “Knowledge Engineering for Medical Vocabularies Using Large Language Models” published in AMIA (2026).
Template Awareness
General AI will write narrative paragraphs. It strings sentences together chronologically, often burying key findings in a large block of text.
Specialty‑specific AI, however, understands the architecture of a clinical note. It knows that the HPI belongs in one section, the ROS in another, and the Physical Exam in a third.
For psychiatry, it can output directly in DAP or BIRP format. Additionally, in orthopedics, it structures the MSK exam with laterality, strength, and provocative tests in a predictable, billable order.
Benefits of Specialty-Specific AI Clinical Notes
- Higher First-Pass Accuracy: Clinicians spend less time editing a specialty-trained AI note than they do on a generic output (which requires a lot more review/editing time).
- Better Medical Coding Support: The model automatically highlights elements that support level 4 or 5 billing, saving you from missed revenue.
- Reduced Hallucinations: Because the model has seen thousands of real notes from your field, it hallucinates terms less often.
How to Evaluate an AI Clinical Note Tool for Your Practice
Before signing a contract with any AI scribe vendor, ask these three questions:
- Question 1: Does the tool provide specialty-specific templates (e.g., your exact ROS checklist or your preferred procedure note format)?
- Question 2: Can you train the AI on your personal writing style (passive vs. active voice, abbreviation preferences, or specific phrasing for recurring diagnoses)?
- Question 3: Does the output integrate with your specific EHR billing requirements (including ICD-10 specificity modifiers and E&M coding calculators)?
If the answer to any of these is "no," the tool will likely cost you more time than it saves
Conclusion
Basic AI note tools convert speech to text efficiently. However, they often miss the clinical nuance that specialty practice requires. A basic model may not distinguish between a provocative test finding and routine discomfort, nor recognize that lesion morphology guides surgical decisions. Specialty‑specific note tools address this gap by learning the vocabulary, structure, and coding expectations of individual fields such as dermatology, orthopedics, cardiology, and psychiatry. For practices seeking documentation that supports both patient care and reimbursement, an AI clinical note tool is a practical consideration worth evaluating.