



The year 2026 marks a turning point. After years of skepticism, clinicians are no longer asking if an AI medical scribe can replace a human scribe; they’re asking which visits it works best for. This article synthesizes what clinicians now say about accuracy, trust, workflow satisfaction, and the non‑negotiable physician review step. Here’s where AI scribes win, where humans still lead, and how hybrid workflows are reshaping modern practice.
What Is an AI Scribe?
An AI medical scribe is an ambient documentation tool that uses three layers of technology: speech recognition, large language models (LLMs), and medical logic layers tuned to clinical vocabulary. Unlike traditional dictation software, an AI scribe runs passively in the background during a patient visit, converting the natural conversation between clinician and patient into a structured clinical note in real time.
Key Capabilities in 2026
Today’s AI scribes have matured significantly beyond simple transcription. Key capabilities include:
- Multi-Speaker Diarization: The AI can distinguish among the clinician, patient, and family members, correctly attributing statements even during overlapping speech or interruptions.
- Specialty-Specific Templates: Whether you’re in orthopedics, dermatology, psychiatry, or cardiology, the AI learns to format notes according to specialty standards (e.g., ROS, physical exam, A&P) and can be customized to your personal style.
- EHR Integration: Notes are pushed directly into your EHR (Epic, Athena, Cerner, etc.) as a structured encounter.
- Real-time Editing: Some platforms allow clinicians to make voice commands without touching a keyboard.
What Is a Human Scribe?
A human scribe is a trained individual who documents patient encounters in real time, either in the examination room or remotely via a secure audio/video feed. In 2026, human scribes still fall into three main categories:
- Live in-Room Scribes: Often pre-med students, medical assistants, or dedicated scribe employees who sit in on visits, type directly into the EHR, and free the clinician to focus on the patient.
- Virtual Scribes: Remote workers who listen to a secure audio feed and build the note in real time, then push it to the EHR for review.
- Float Scribes: Shared among multiple clinicians in a practice to cover peak hours or complex encounters.
Human scribes act as an extension of the clinician’s memory and hands, capturing details the clinician might otherwise have to type or dictate later.
How the AI vs. Human Scribe Debate Has Shifted in 2026
Just a few years ago, most clinicians viewed AI scribes as a promising but risky experiment. Early systems suffered from:
- Frequent hallucinations (invented symptoms, wrong laterality).
- Poor handling of medical terminology and medication names.
- No clear HIPAA guidance or EHR integration.
The Shift in 2025
These major changes accelerated adoption in 2025:
- EHR-native Integrations: Major EHR vendors (Epic, Oracle Cerner, Athenahealth) began embedding ambient AI scribes directly into their workflows, eliminating copy-paste issues.
- Several large health systems published pilot data demonstrating non-inferiority to human scribes for low- to moderate-complexity visits.
Relevant Study: “Ambient Documentation Technologies Reduce Physician Burnout and Restore ‘Joy’ in Medicine” —Mass General Brigham, Q3 2025.
2026: Pragmatic Acceptance
Today, the debate has fundamentally shifted. Clinicians are no longer asking “Should I try an AI scribe?” but rather:
- “Which visits are safe to delegate entirely to AI?”
- “How do I build a hybrid workflow that maximizes efficiency without compromising safety?”
- “What’s my liability if an AI hallucinates a finding I miss in review?”
Where AI Scribes Are Winning: Efficiency, Burnout, and Patient Connection

AI scribes consistently outperform on these three key fronts:
Area | AI Scribe | Human Scribe |
|---|---|---|
Time saved daily | More (up to 2 hours on charting) | Less |
Burnout reduction | Greater | Moderate |
Patient connection | Higher | Lower |
Key Takeaways
- AI scribes save clinicians more time each day than human scribes.
- Burnout improves more with AI scribes.
- Patient connection improves because clinicians are less distracted by typing.
- Human scribes still lead slightly on accuracy.
See how much time you can save with an AI scribe.
Where Human Scribes Still Have the Edge
Despite AI scribes gaining ground in 2026, human scribes have distinct advantages in specific clinical scenarios:
- Complex, High-Acuity Encounters: For trauma, complex care coordination, or end-of-life discussions, most clinicians still prefer a human scribe.
- Multilingual and Dialect Nuance: AI scribes struggle with heavy accents, code-switching (mixing languages mid-sentence), or rare dialects.
- Dynamic Question-Answering: A human scribe can interrupt politely to ask: “Wait, did you say 5 mg or 50 mg?”
The Hallucination Problem: Why AI Scribe Notes Still Need a Physician Review Step
Hallucinations are the single biggest safety risk with AI scribes. Every clinician using an AI scribe must understand what they look like and why review is non‑negotiable.
Mandatory Physician Review Workflow
Because hallucinations still happen, every AI‑generated note must be reviewed by a physician before signing. This is not optional.
Look specifically for:
- Symptoms or findings you never said.
- Laterality errors.
- Lab values or medications that sound unfamiliar.
For more information, see how AI scribe works during patient visits.
AI vs. Human Scribes by Specialty: What Clinicians Are Choosing
The table below shows which type each specialty is more likely to choose in 2026.
Specialty | Most likely to choose |
|---|---|
Dermatology | AI scribe |
Primary care | AI scribe |
Orthopedics | AI scribe |
Emergency medicine | Hybrid |
Psychiatry | Hybrid |
Pediatrics | Hybrid |
General surgery | Human scribe |
Find the right fit for your specialty with the best AI scribe tools in 2026.
The Hybrid Workflow: How Clinics Are Using Both AI and Human Scribes
Most forward‑thinking clinics in 2026 no longer choose between AI and human scribes. Instead, they use both, each for what it does best.
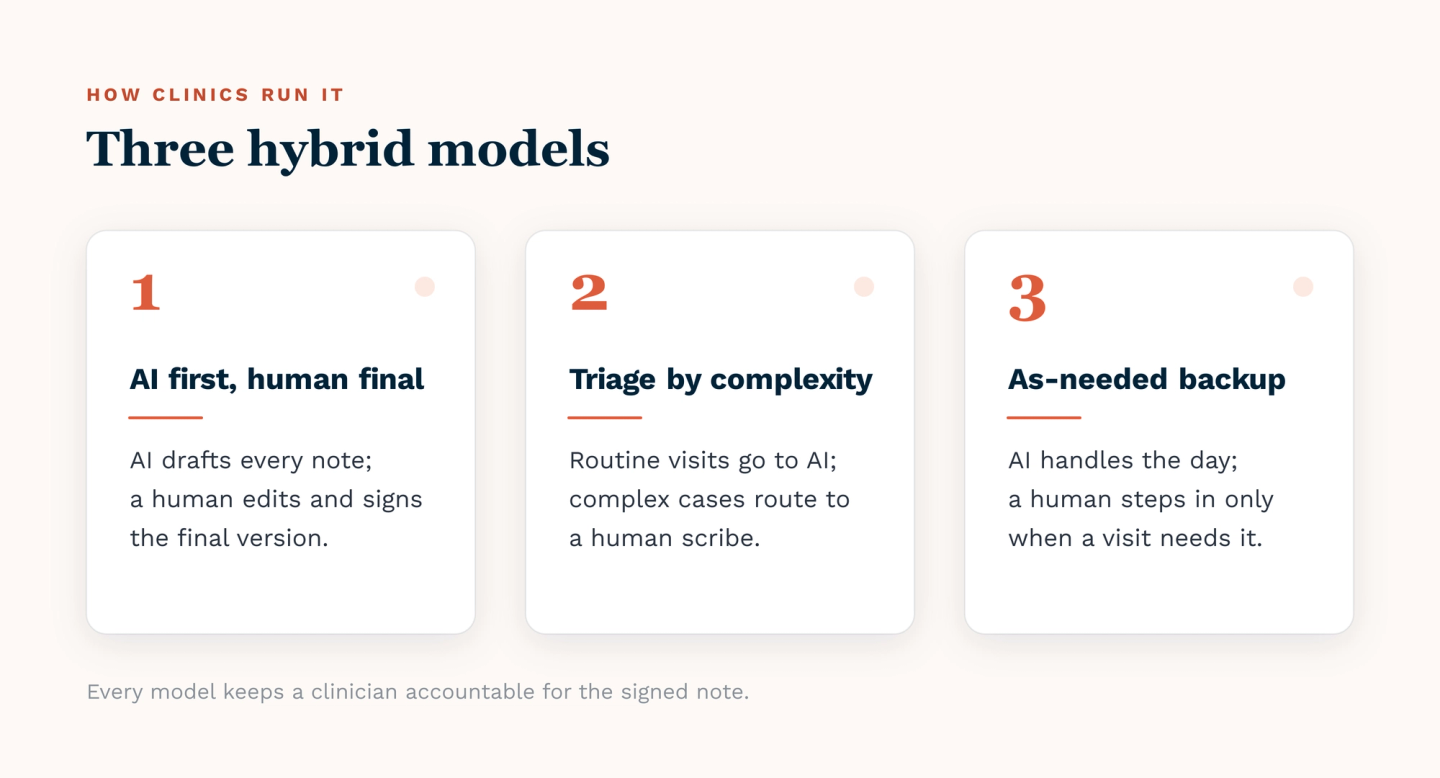
Model 1: AI First, Human Final
The AI scribe generates the first draft. A human scribe (often virtual) reviews, corrects, and polishes the note before the physician signs.
Best for: Clinics that want AI speed but still want a human safety net.
Model 2: Triage by Visit Complexity
Simple visits (colds, rashes, medication refills) go to AI scribes. Complex visits (new cancer diagnosis, family meetings, trauma follow‑ups) go to human scribes.
Best for: Practices with a wide mix of patient acuity.
Model 3: As-Needed Human Backup
The AI scribe handles 90% of visits. A human scribe is on call for specific patients, difficult encounters, or when the clinician simply wants an extra set of ears.
Best for: Solo practitioners and small groups who cannot afford a full‑time human scribe.
How Clinicians Are Evaluating AI Scribes Before Switching
In 2026, smart clinicians don't just sign up for the first AI scribe they hear about. They run a structured evaluation to ensure safety, accuracy, and fit for their practice.
A Basic Workflow Fit Test
Run the AI scribe alongside your current workflow (human scribe or self‑documentation) for 5 to 10 patient visits. Compare the AI‑generated notes against your usual notes side by side. Look for:
- Missing information.
- Invented details (hallucinations).
- Formatting and template fit.
This simple test reveals whether an AI scribe is ready for your patients.
HIPAA, Compliance, and Data Privacy: What Changes When You Switch to an AI Scribe
Switching from a human scribe to an AI scribe changes your compliance responsibilities. Here is what clinicians need to know in 2026.
Compliance Area | Human Scribe | AI Scribe |
|---|---|---|
Business Associate Agreement (BAA) needed | No (employee) | Yes |
Audio recorded and stored | No | Yes (audio is deleted after the session is recorded) |
Patient consent required | Yes | Yes |
Less Charting, More Care: How Twofold Gives Clinicians Back Their Time
Three ways Twofolds AI medical scribe for clinicians helps you move from hours of charting to more time with patients and family.
- Ambient Documentation: Twofold listens to your conversation with your patient, then generates a complete, specialty-appropriate clinical note in seconds.
- Seamless EHR Integration: Notes flow directly into your existing EHR (Epic, Athena, Cerner, and others) with a simple copy-paste. No formatting chaos, just a clean note ready for your final review.
- Built for Safety: Twofold includes a full audit trail and a Business Associate Agreement (BAA). Your data is never used to train our models. You stay compliant and in control.
Conclusion
In 2026, the choice between AI and human scribes is no longer about which is better overall, but which is better for each visit. AI scribes win on efficiency, burnout reduction, and patient connection. Human scribes still lead for complex, high‑acuity, or linguistically challenging encounters. Most clinicians now use a hybrid model. The non‑negotiable rule: physician review of every AI‑generated note. If you are ready to save time without sacrificing safety, Twofold provides a compliant, accurate, and affordable AI scribe.