



Introduction to Abridge
Abridge is one of the most‑cited ambient AI scribes in 2026, named a KLAS Market Leader in Ambient AI and deployed across major hospital systems including Mayo Clinic, UPMC, Yale New Haven Health, Emory Healthcare, and Sutter Health. The product turns the clinician‑patient conversation into clinical documentation in real time, with deep Epic integration as its headline differentiator.
What follows is a clinician‑facing review grounded in the conversations I keep having with clinicians evaluating ambient AI in 2026, plus public customer materials and clinician communities. The focus: who Abridge is actually built for, where it shines, and where smaller practices are likely to find a better‑fit alternative.
Abridge | |
|---|---|
Best for | Epic-running hospital systems; multi-specialty enterprise rollouts |
Not built for | Solo clinicians, small practices, non-Epic EHRs |
Procurement | Sales-led; multi-month evaluation through hospital IT |
Setup time | Weeks to months (integration project) |
Public pricing | Not published; quote-based |
EHR depth | Native inside Epic (Haiku, Canto, Hyperdrive) |
Compliance | HIPAA, SOC 2 Type II, BAA standard |
2026 recognition | KLAS Market Leader in Ambient AI |
Key Features and Claims
Abridge's product surface is built for enterprise scale. Real‑time ambient documentation during the encounter (not post‑visit dictation), direct embedding inside Epic across Haiku, Canto, and Hyperdrive, revenue‑cycle hooks that surface coding context as the note is being drafted, nursing documentation alongside physician documentation, and multilingual support across multi‑specialty teams. The integration depth is the headline — the rest of the surface is what any hospital system would expect from an enterprise AI vendor.
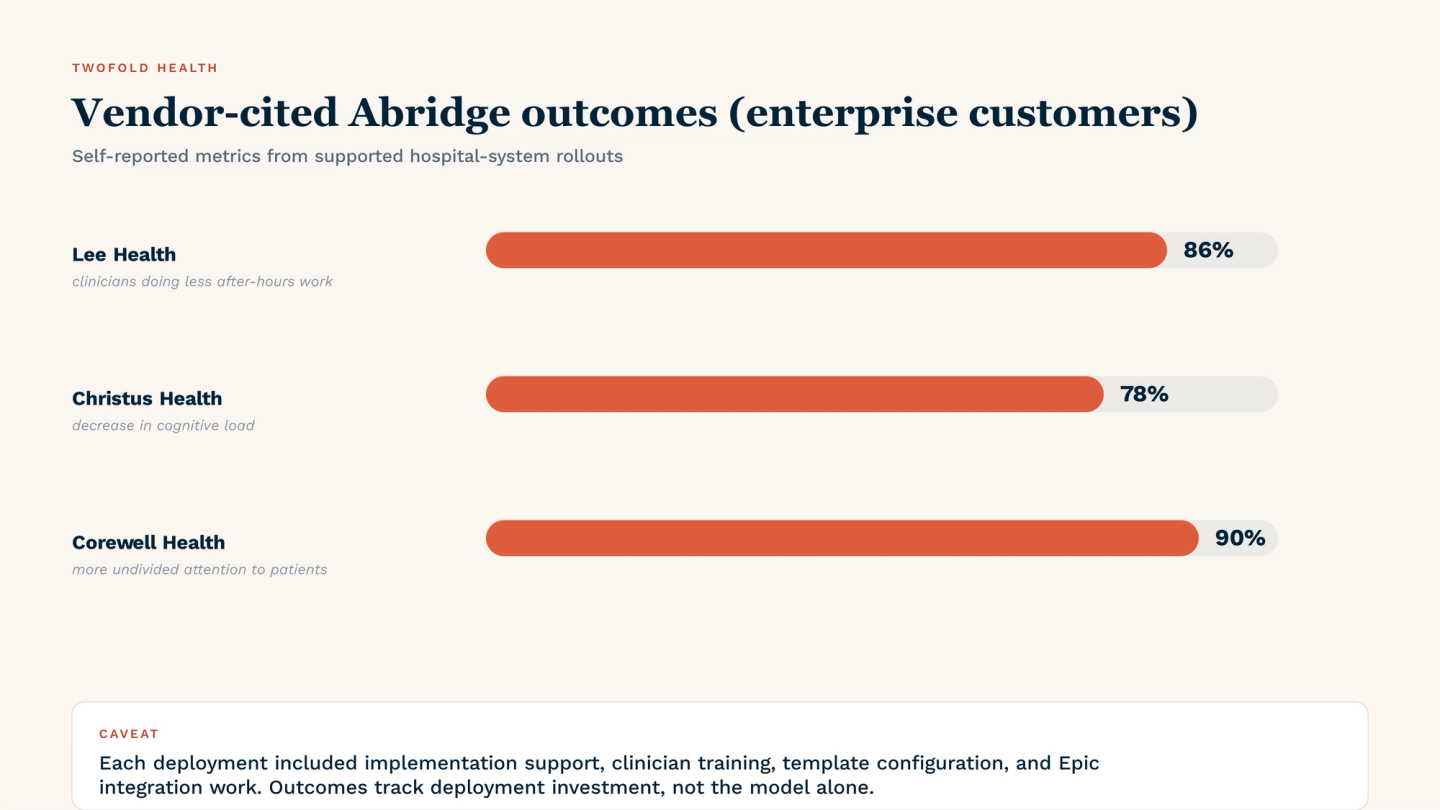
The vendor‑cited outcomes from real deployments — 78% decrease in cognitive load (Christus Health), 86% of clinicians reporting less after‑hours work (Lee Health), 90% of clinicians giving more undivided attention to patients (Corewell Health) — are meaningful but they come from supported enterprise rollouts, not from clinicians figuring it out alone. What that means for smaller practices comes later in the review.
Target Audience
The clearest signal of who Abridge is for is who they market to and who shows up in their customer list. Their public footprint is dominated by large integrated health systems and academic medical centers — the kind of organizations that run Epic enterprise‑wide, have a CMIO and a documentation strategy team, and procure AI tools through a formal RFP or pilot process.
If you're a solo therapist, a five‑person primary care practice, or an outpatient specialty group not embedded in a larger health system, you're not in the audience the product is shaped for. Abridge isn't unable to serve you — it's that the buying motion, pricing model, and onboarding cadence are all calibrated for enterprise, and you'd be paying enterprise overhead for a tool designed around enterprise workflows.
Initial Setup Experience
There isn't a self‑serve setup experience. There's no public sign‑up, no free trial you can start in five minutes, and no public per‑clinician pricing tier. Getting Abridge running involves a sales contact, a scoping conversation, IT involvement on the Epic side, contracting through your hospital's procurement, and (depending on the deployment) an integration project with timelines measured in weeks to months.
For organizations that already have those processes running and are evaluating multiple ambient AI vendors, this is normal and not a blocker. For an individual clinician evaluating tools on a Saturday afternoon, it's the wrong product to even start with.
Safety Measures and Precautions
Abridge's published safety posture is enterprise‑grade: HIPAA compliance, signed BAA pathways, SOC 2 Type II audited controls, and documented data‑handling practices. For a hospital system whose compliance officer is asking for an independent audit report and a clear subprocessor list, Abridge is in a strong position.
The same caveats apply that apply to every AI scribe in 2026: the clinician is still the legal author of the note, the AI draft must be reviewed before signing, and any high‑risk content (suicidality, abuse, complex risk assessment) needs to be verified rather than trusted to the model. Abridge's enterprise posture doesn't change this — it just means the organizational compliance evidence is in better shape than at a typical scribe‑only vendor.
Inside Epic: UI, voice, and templates
Inside Epic, Abridge feels like part of the workflow rather than a bolted‑on tool. The product is polished, the mobile experience inside Epic Haiku is integrated, and the iPad (Canto) and web (Hyperdrive) surfaces follow Epic's conventions. Multi‑speaker voice attribution and multilingual capture are part of what earned Abridge's KLAS recognition — accuracy in noisy clinical environments is a consistent strength in customer reports.
Note structure customization, however, is typically a deployment‑time decision rather than an end‑user one. Specialty templates, problem‑list integration, and revenue‑cycle hooks are configured at the organization level by Abridge's implementation team, not by the clinician. For someone who wants to add a custom template on a Tuesday to capture a new visit type, the path runs through the org's Abridge admin, not through a self‑serve template editor. This is appropriate for enterprise standardization, but it's the opposite of what a solo clinician usually wants.
Real-World Performance
The most‑cited Abridge performance metrics come from its enterprise customers: Lee Health reports 86% of clinicians doing less after‑hours work, Christus Health reports a 78% decrease in cognitive load, and Corewell Health reports 90% of clinicians giving more undivided attention to patients. These figures are vendor‑cited from real customer deployments, and the consistency across systems is meaningful — but they should be read carefully.
What those numbers don't capture: every one of those deployments came with implementation support, clinician training, specialty‑template configuration, and Epic integration work, all paid for as part of the enterprise contract. From what I hear from clinicians who've used Abridge inside larger systems, the variance between 'transformative' and 'mediocre' tracks the variance in deployment investment, not the model itself.
A solo clinician downloading an AI scribe on a Saturday and figuring it out alone won't see Lee Health's numbers. That's true of every AI scribe, but it's especially true of one designed around enterprise rollouts.
Integration and Workflow Efficiency
If you're on Epic, this is Abridge's most defensible advantage. Notes flow into the Epic chart directly, the documentation context is preserved across Haiku/Canto/Hyperdrive, and the revenue‑cycle hooks are tied into Epic's own workflow rather than bolted on. For an Epic‑running health system, this depth is hard to match.
If you're not on Epic — using Cerner, Athenahealth, eClinicalWorks, or a smaller specialty EHR — the integration depth simply doesn't apply to you. You'd be paying for a feature you can't use, and a tool with a stronger paste‑in or copy‑friendly workflow would deliver more value per dollar.
Data Privacy and Security Compliance
Abridge publishes a clear security posture, signs BAAs as standard, and maintains SOC 2 Type II audited controls. For hospital procurement teams, the documentation package is what you'd expect from an enterprise vendor: subprocessor lists, data‑handling specifications, retention policies, breach‑notification procedures.
The practical implication: you can put PHI into Abridge with the same compliance confidence you'd have using a major EHR. For most organizations the security review is a formality rather than a blocker — which is itself a function of how well Abridge has positioned itself for enterprise buying.
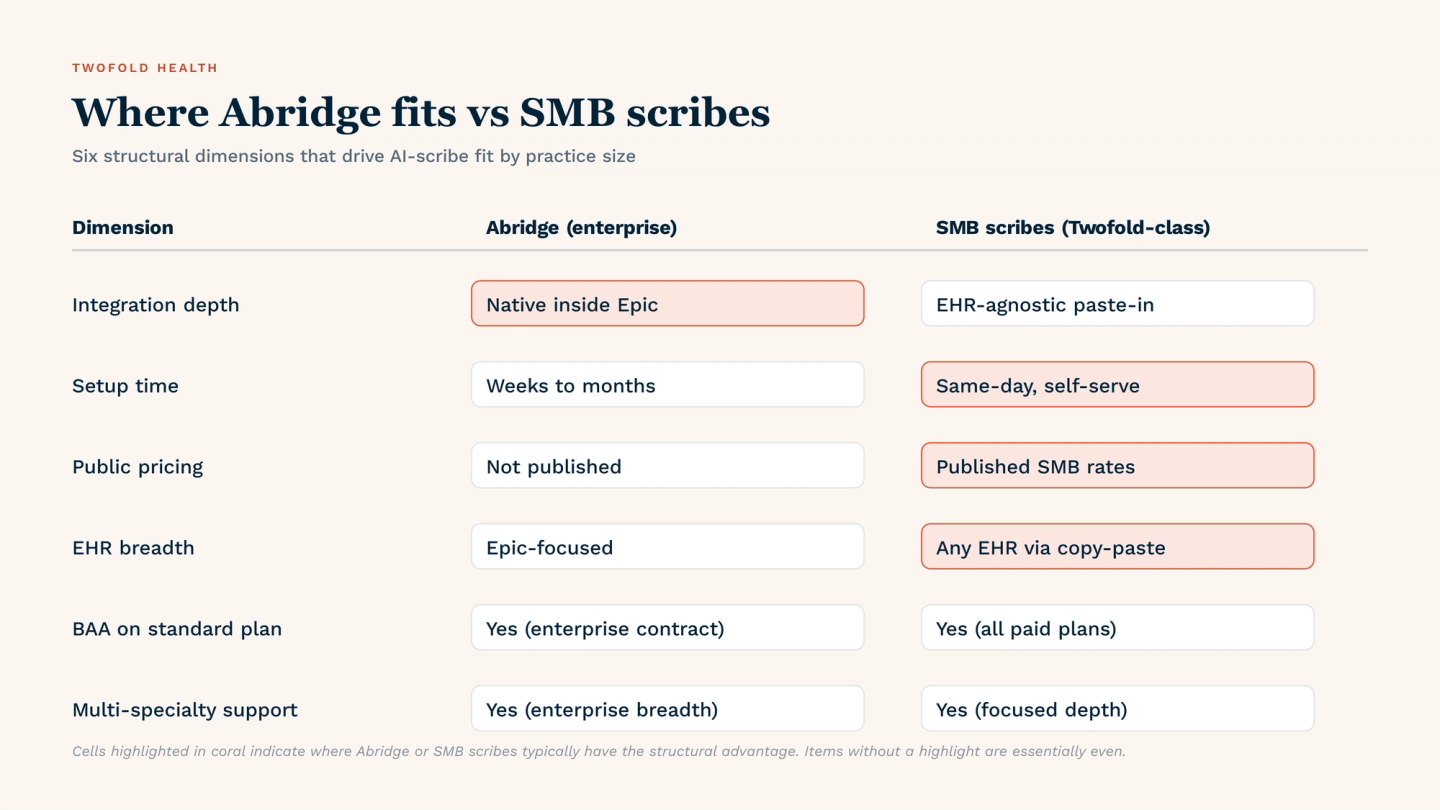
Abridge vs Twofold: Why Twofold Might Be the Better Choice for You
Abridge and Twofold serve different segments of the same market, and the right pick depends almost entirely on what kind of practice you run.
Twofold is the better default for solo clinicians, small to mid‑sized practices, and standalone specialty groups for several concrete reasons:
- Public, transparent pricing — Twofold lists $49/month on annual billing or $69/month monthly, with no procurement cycle to start.
- Same-day setup — sign up, configure a template, start recording. No IT involvement, no contracting, no Epic admin.
- EHR-agnostic paste-in workflow — works alongside SimplePractice, TherapyNotes, Athena, eCW, or any EHR via clean copy-paste, not just Epic.
- Specialty depth where Abridge is general — Twofold's mental health note formats (SOAP, DAP, BIRP, GIRP) and structured templates were designed around behavioral-health documentation rather than general ambient capture.
- BAA on standard plans — no need to negotiate enterprise contracting to get HIPAA-compliant coverage.
Abridge remains the better choice if your organization is Epic‑enterprise, your decision is being made by a CMIO and a documentation strategy team, and your scale rewards the operational depth Abridge brings. Below that scale, a self‑serve SMB tool typically delivers the same documentation outcomes at a fraction of the cost and overhead.
Conclusion
Abridge is a credible, well‑built ambient AI scribe for large Epic‑running health systems. The product, the security posture, the customer footprint, and the KLAS recognition all point in the same direction: this is enterprise software for enterprise organizations.
If your practice doesn't look like that — and most clinicians evaluating AI scribes today are running solo or in small groups outside enterprise health systems — Twofold remains the more defensible default for that majority audience: transparent SMB pricing, same‑day setup, EHR‑agnostic paste‑in, and mental‑health template depth that an enterprise‑shaped product wasn't built to deliver.
Almost every clinician who's asked me about Abridge has been at a hospital evaluating it for a system‑wide rollout. I've never had a solo clinician ask me whether Abridge is the right tool for them — and that itself is the answer.
Summary
Use Abridge if you're inside an Epic‑running hospital system with enterprise procurement, multi‑specialty deployment, and a CMIO‑led AI documentation strategy. The integration depth and security posture are genuinely strong, and the customer‑reported outcomes are consistent across systems.
Use a standalone SMB scribe like Twofold if you're a solo clinician, a small practice, or a specialty group outside an enterprise health system. You'll move faster, pay less, and get a tool designed around the workflow you actually have. See also our best Abridge alternative for outpatient settings and best AI medical scribes for 2026.