



Brief Answer
AI scribes can be very helpful in family medicine when you have high visit volume, lots of multi problem encounters, and a clear review routine. They are less helpful if your main issue is schedule design, inbox overload, or very sparse documentation expectations.
They are usually worth it if you use them to capture a short, focused clinical story and then review key sections only, instead of rewriting the entire note. They are overhyped if you expect them to magically remove all charting work without any review or adaptation of your own workflow.
The Longer Answer
Here we look at the question from four angles: where AI scribes shine, where they struggle, what the financial trade off looks like, and how to run a low risk trial.
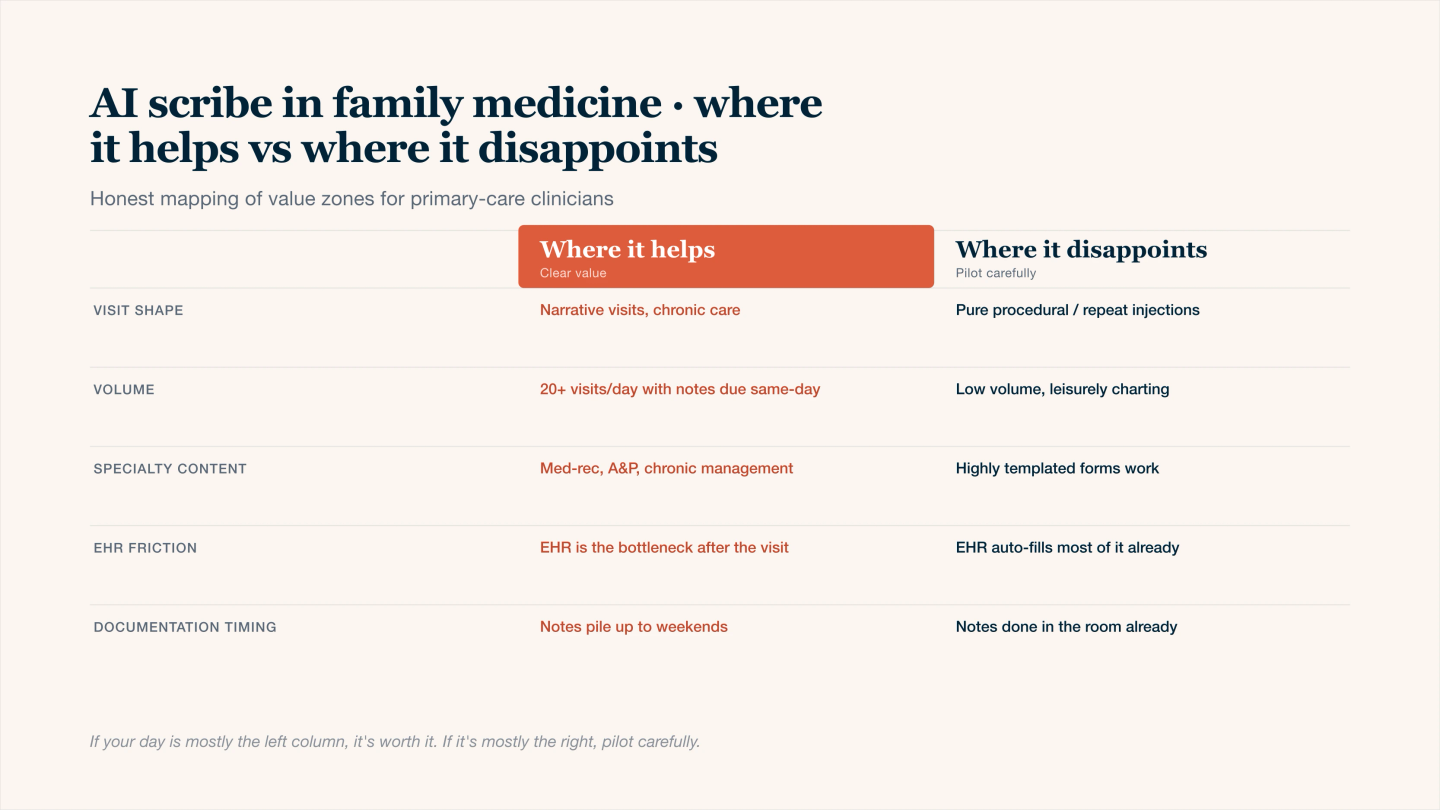
AI scribe in family medicine — where it earns its keep, and where it doesn't.
1. Where AI scribes usually help in family medicine
Typical high value situations:
- Many visits with three or more active problems
- Complex polypharmacy with frequent med adjustments
- Chronic disease management with repeated lab review
- Clinicians who think out loud and summarize decisions in the room
- Clinics that expect complete MDM, risk, and quality documentation
In these contexts, AI can capture your spoken reasoning and turn it into a structured note so you are editing instead of building from a blank page.
Table: Use cases where value is often clear
Scenario | How AI scribe helps | What you still do |
|---|---|---|
Multi problem chronic follow up | Drafts A and P per problem, with labs and monitoring | Confirm meds, goals, and follow up timing |
Same clinician, high daily volume | Keeps notes moving during the day | Quick review of meds, risk, and medical necessity |
Preventive plus chronic in one visit | Separates wellness items from problem based plans | Check coding support and HM completion |
Teaching or team based visits | Captures long discussions that are hard to type | Trim content and highlight final decisions |
If you often spend several minutes per note reconstructing conversations, AI scribes can shift most of that time to a short review.
2. Where AI scribes tend to disappoint
AI scribes do not fix everything:
- Overloaded templates and local policies that force very long notes
- Schedule templates that leave no time between visits at all
- Inbox tasks and messaging volumes that are unrelated to charting
- Situations where you rarely verbalize reasoning or decisions
They can also disappoint if you let the model produce long narrative text that you then feel obliged to line edit. The more you ask for exhaustive detail, the more you will need to proofread.
Table: Common pitfalls
Pitfall | What it looks like | Better approach |
|---|---|---|
Overly long drafts | Pages of narrative for simple acute visits | Use a short visit prompt and a slim template |
Copy like notes across visits | Very similar MDM wording each time | Add visit specific vitals, labs, and functional impacts |
Weak review habits | Signing without checking orders or risk language | Fixed two minute review pattern per note |
Misaligned expectations | Expecting zero click or zero review charting | Aim for shorter, more focused review instead |
3. Is it financially worth it
A simple way to think about value is to compare subscription cost with hours of charting saved and how you use that regained time.
Table: Rough time and cost frame
Factor | Example numbers |
|---|---|
Patients per day | 18 to 24 |
Minutes saved per note | 3 to 6 once the workflow is dialed in |
Time saved per day | About 1 to 2 hours |
Time saved per month | Roughly 15 to 30 hours |
Typical AI scribe cost | Similar to or less than one half day of your revenue |
The value feels real if that time turns into earlier finish times, room for admin you were not doing, or space to add a few visits per week without burnout.
4. Safety, accuracy, and compliance
Non negotiables for family medicine:
- Use a vendor that signs a Business Associate Agreement and states they are HIPAA compliant
- Confirm how audio and text are stored, encrypted, and de identified
- Have a standard process for late entry, corrections, and addenda
- Keep a human in the loop: you decide what goes into the chart
For clinical accuracy, most family medicine clinicians focus their review on patient identity, medications and orders, risk and safety language, and assessment and plan per problem. The rest can usually be scanned quickly for obvious mismatches.
5. How to trial an AI scribe without disruption
A simple three week trial pattern:
- Week 1: Use it for a subset of visits only, such as established chronic follow ups. Compare time spent per note with and without the tool.
- Week 2: Expand to most of your schedule, keep a two minute review rule, and notice evening charting time.
- Week 3: Adjust your prompts and templates to remove fluff and focus on problem based A and P, medical necessity, and quality metrics.
If after three weeks you are not saving at least an hour per day or you dislike the notes, it is reasonable to call it not worth it for your situation.