



Brief Answer
Yes, some clinicians regret trying an AI scribe, but usually not because the concept is bad. Regret typically comes from a mismatch between the tool and the workflow, unrealistic expectations, or poor setup. The biggest drivers are overly long drafts, too much review time, weak specialty fit, or unclear compliance steps. When clinicians start with a tight template, clear prompts, and a two minute review routine, regret rates drop a lot.
The Longer Answer
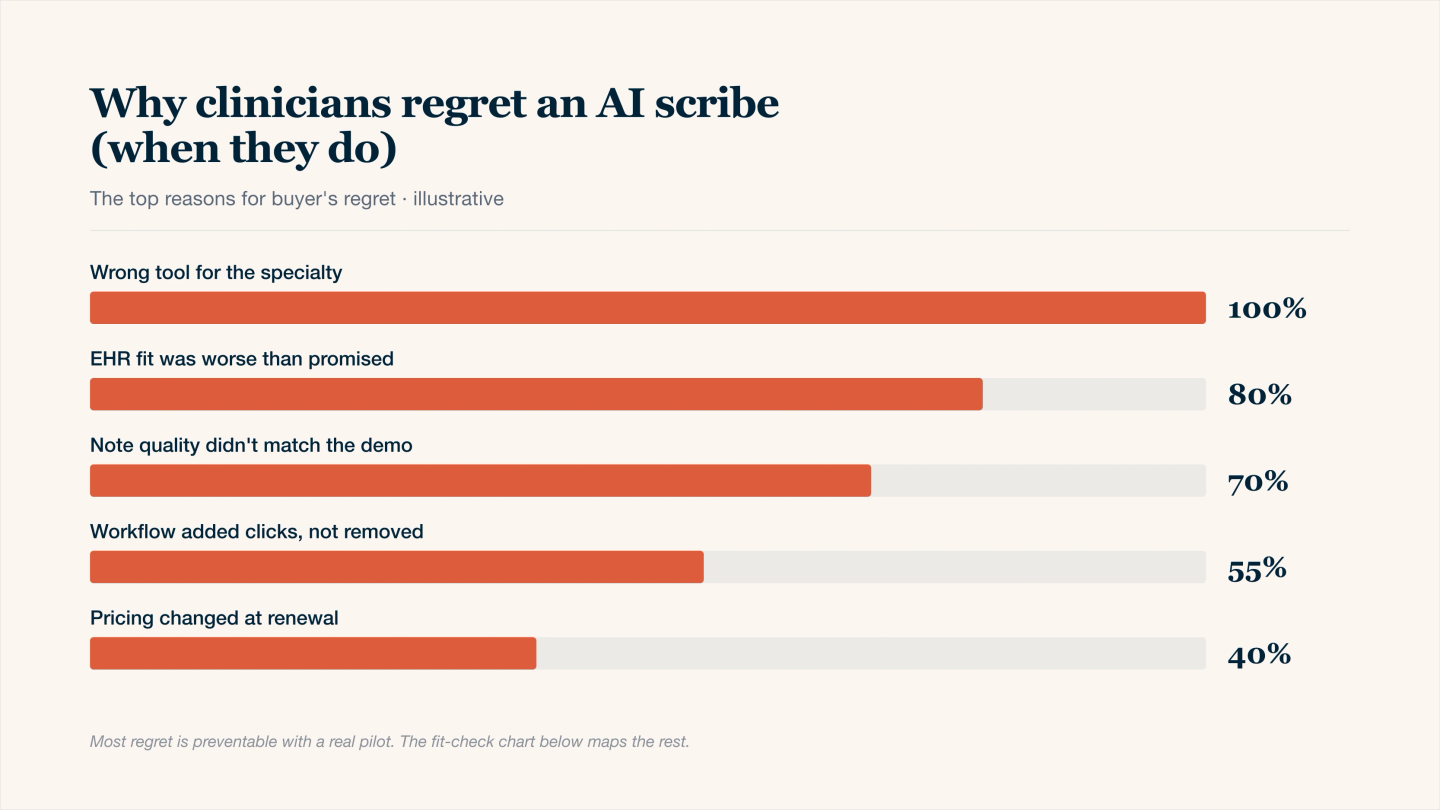
Why clinicians regret an AI scribe — five preventable mismatches.
1. What regret usually looks like
Clinicians who stop using an AI scribe tend to say one of these:
- “It saved time at first, but drafts became too verbose.”
- “I still had to rewrite half the note.”
- “It missed key clinical decisions or risk language.”
- “My EHR integration was clunky so it added steps.”
- “I was not fully confident about compliance.”
These are solvable, but only if you know what to watch for.
2. The main reasons people regret AI scribes
Here is a plain list of the most common causes, ordered by how often they show up in real clinics.
Reason | What it causes | Early warning sign |
|---|---|---|
Too much text | Editing takes as long as writing | Notes feel like full transcripts |
Weak template fit | Missing key sections, wrong ordering | You keep moving text around |
Low signal capture | AI makes assumptions or fills gaps incorrectly | Draft includes details you did not say |
No fixed review habit | Anxiety or errors after signing | You feel unsure every time |
EHR friction | Copy paste or field mapping slows you down | You dread the final step |
Cost without clear ROI | Subscription feels like a tax | You are not saving at least 45 minutes a day |
Notice that most of these are about process, not about the model itself.
3. A quick “fit check” before you commit
Use this short self test. If you answer yes to most, regret is less likely.
- I see enough volume or complexity that saving even 3 minutes per note matters.
- I am willing to review meds, risk, and plan before signing.
- I can speak a short summary or let the tool ambient capture my key decisions.
- My notes follow a repeatable structure I can standardize.
- I know my compliance requirements and need a BAA.
If most are no, you might still benefit, but you may need a lighter tool or a tighter rollout.
4. What prevents regret in practice
Instead of “trust the AI,” the clinicians who stick with it do a few simple things.
Keep the prompt narrow
Focus on problems, decisions, and plan. Avoid “capture everything.” Less input noise creates shorter drafts.
Use problem oriented sections
For primary care, make sure the plan is per problem. For therapy, make sure you name interventions and response.
Set a review ceiling
A realistic habit is one to two minutes per note, prioritizing identity, meds, orders, risk, and assessment and plan.
Measure outcomes, not vibes
Track time spent after clinic for two weeks before and after. If you are not saving meaningful time, change the setup or stop.
5. When regret is actually a good decision
Sometimes stopping is correct. It is reasonable to pause or cancel if:
- Your day is low volume and documentation is already fast.
- You hate speaking your reasoning out loud and do not want ambient capture.
- Your clinic expects ultra minimal notes and AI drafts feel like overkill.
- Your EHR workflow adds friction you cannot remove.
AI scribes are not universal. The goal is fit, not ideology.