



Brief Answer
SOAP notes usually take too long when you are trying to capture the entire conversation instead of the clinical story, using templates that are too heavy, and starting from a blank screen for each section. The goal is not more words. It is clear medical necessity, a small number of focused findings, and a specific plan per problem.
If you tighten what each SOAP section is responsible for and use sentence stems or AI to fill the structure, you can usually get most notes down to about three to seven minutes without losing quality.
The Longer Answer
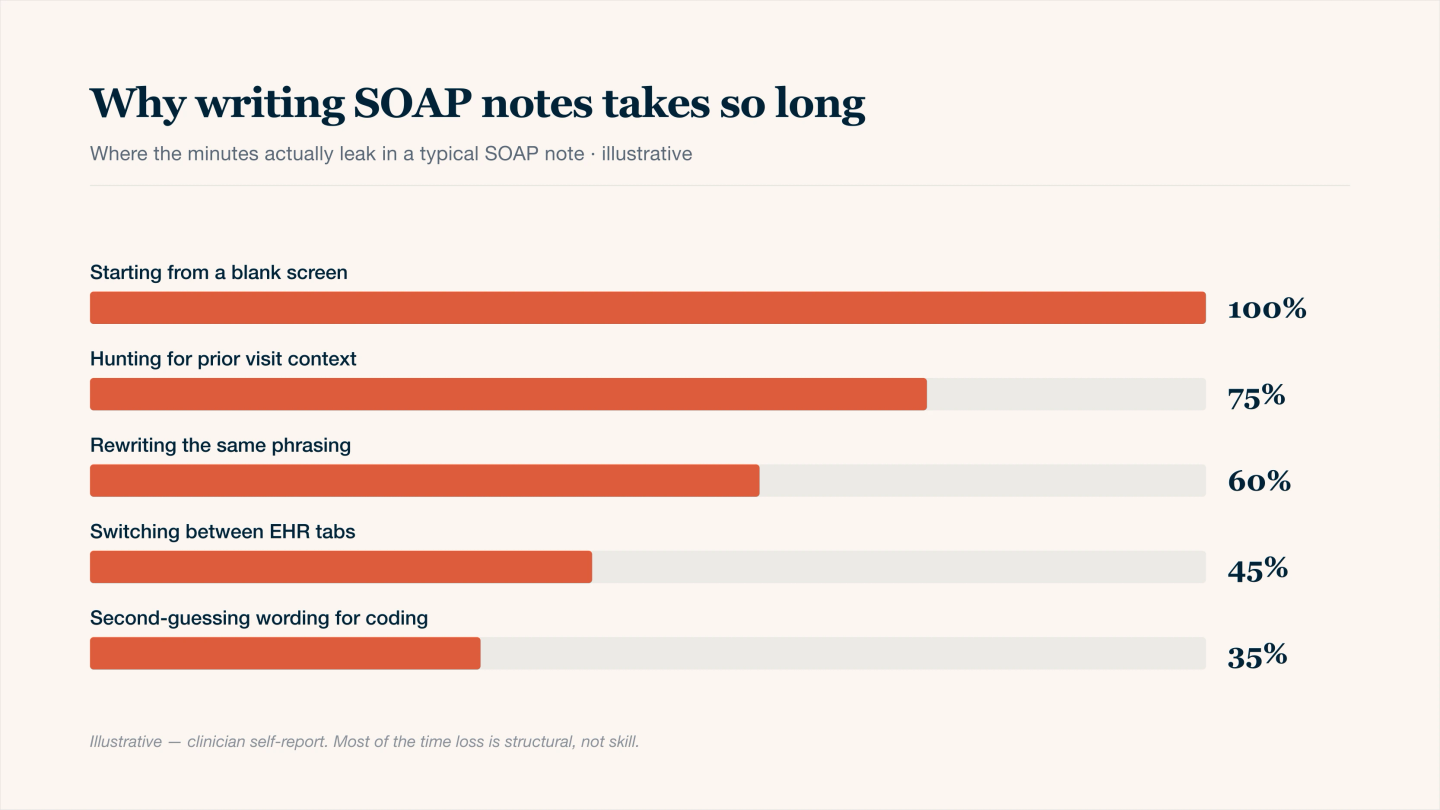
Where the minutes actually leak in a SOAP note — most slowness is structural.
1. Quick self check: why your SOAP notes are slow
Use this as a mirror.
Pattern you notice | Likely cause | What it does to SOAP notes |
|---|---|---|
Writing long narratives of what was said | Treating Subjective as a transcript instead of a summary | Subjective swells and is hard to skim |
Rewriting the entire exam every time | Copy forward habits and fear of missing something | Objective becomes a wall of text |
Struggling to phrase Assessment | Trying to document every thought process | Assessment becomes vague or very long |
Delaying Plan until later | Not deciding next steps during the encounter | Plan feels hard to start and easy to avoid |
Editing the template more than the note | Template has too many fields and auto text | You spend time cleaning instead of documenting |
If two or more of these feel familiar, the problem is structure and expectations rather than your ability.
2. Where the time usually leaks in SOAP
Subjective (S)
- Trying to retell the full dialogue.
- Including history that does not change decisions today.
- Mixing in your interpretation instead of sticking to patient report.
Objective (O)
- Auto inserted full normal exams that you then adjust line by line.
- Re documenting every stable chronic finding at each visit.
- Copy forward that you then need to debug for each encounter.
Assessment (A)
- Overly general wording that you rewrite repeatedly.
- Unclear link between symptoms, function, and diagnosis.
- No consistent pattern for multi problem visits.
Plan (P)
- Writing free form paragraphs instead of brief lists.
- Trying to record every detail of counseling.
- Leaving PDMP checks, labs, or follow up out until the end then hunting for them.
Most of the time, the note is slow because you are deciding what the visit was about while writing. The fastest notes are written after decisions are already clear.
3. What a lean, solid SOAP note actually needs
You can keep this as your personal standard.
Section | Must include | Can be brief on | Example line |
|---|---|---|---|
Subjective | Reason for visit, key symptoms, duration, relevant changes since last time | Exact quotes, full narrative of the session | “Follow up for GAD. Worry about work performance, poor sleep 4 nights per week, one panic episode since last visit.” |
Objective | Pertinent exam findings, vitals, key test results that matter today | Full normal exams unrelated to the problem | “Affect anxious, speech normal rate. BP 142 over 88. Lungs clear. No tremor.” |
Assessment | Diagnosis or working impression, status (improved, unchanged, worse), link to function and risk | Every branch of differential if it does not change the plan today | “GAD with partial response. Ongoing worry affecting concentration at work and sleep onset.” |
Plan | Meds and dose changes, interventions, labs or tests, referrals, risk and follow up | Long prose about education if it does not change decisions | “Increase SSRI to 40 mg daily, review side effects. Continue CBT weekly. No SI. Follow up in 4 weeks.” |
If each section covers these pieces, most insurers and auditors have what they need.
4. Small changes that speed up SOAP without losing quality
You can test these over a single week.
A. Use sentence stems instead of starting from zero
Create three to five stems for each section.
Examples:
- Subjective
- “Today presents for …”
- “Since last visit, reports … with impact on …”
- Objective
- “Exam notable for … otherwise as prior.”
- Assessment
- “[Diagnosis] with [better or worse or unchanged] symptoms, affecting …”
- Plan
- “Will [start or continue or adjust] [med or intervention] because …”
- “Safety: [no SI or HI, or risk and plan]. Follow up in …”
Stems remove decision fatigue about phrasing, which is surprisingly time consuming.
B. Decide in the room, not at the keyboard
At the end of the encounter, say a one or two sentence recap to yourself or the patient:
“Today we focused on medication side effects and updated the dose, you will track sleep and we will check in four weeks.”
When you sit down to write, you are documenting decisions that already exist instead of thinking them through for the first time.
C. Limit time per note based on visit type
Visit type | Reasonable target time for SOAP |
|---|---|
Simple acute, one problem | 2 to 3 minutes |
Routine follow up, one or two problems | 3 to 5 minutes |
Complex multi problem or new patient | 5 to 8 minutes |
If you routinely go beyond these, you are likely including detail that does not change care or billing.
D. Clean your template once, not every day
Take 20 to 30 minutes once to remove extra auto text and unused fields in your SOAP template. Focus on the sections you actually use. A lean template saves minutes every day.