



The healthcare industry is embracing AI scribes to reduce documentation burdens. Yet, while a generic AI tool can draft a passable SOAP note, it often fails at the nuance aspect. A one‑size‑fits‑all format cannot distinguish the distinct differences and needs for pediatric, behavioral health, and primary care documentation. When AI ignores these specialty‑specific rules, it produces clinically inadequate notes. To combat this issue, discover how to adopt distinct frameworks tailored to the unique demands of each discipline with AI SOAP notes.
Why Context Matters in AI SOAP Notes
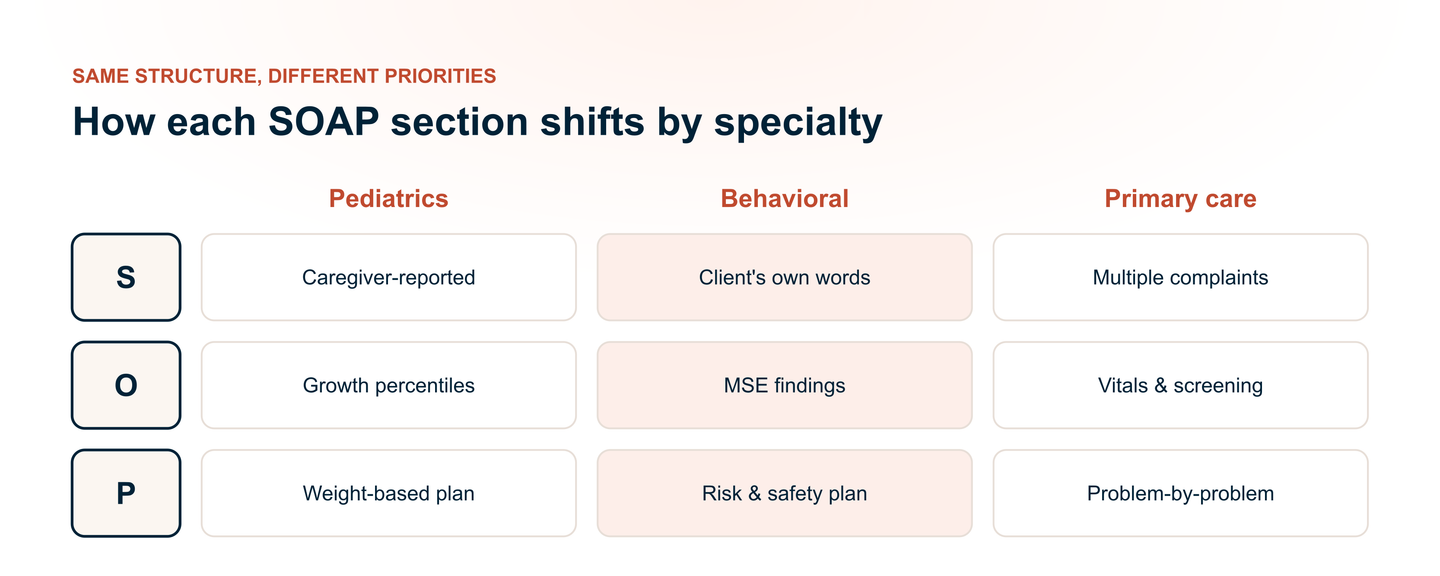
Before diving into specialty‑specific requirements, we must first understand why AI cannot treat all clinical documentation equally. The SOAP format is a universal framework, but the weight and interpretation of each section shift dramatically depending on the patient population and clinical setting. Ignoring these contextual differences creates clinically useless documentation.
The Danger of the "Generic" Note
Generic AI models are trained on vast, diverse datasets, which means they tend to produce "average" notes.
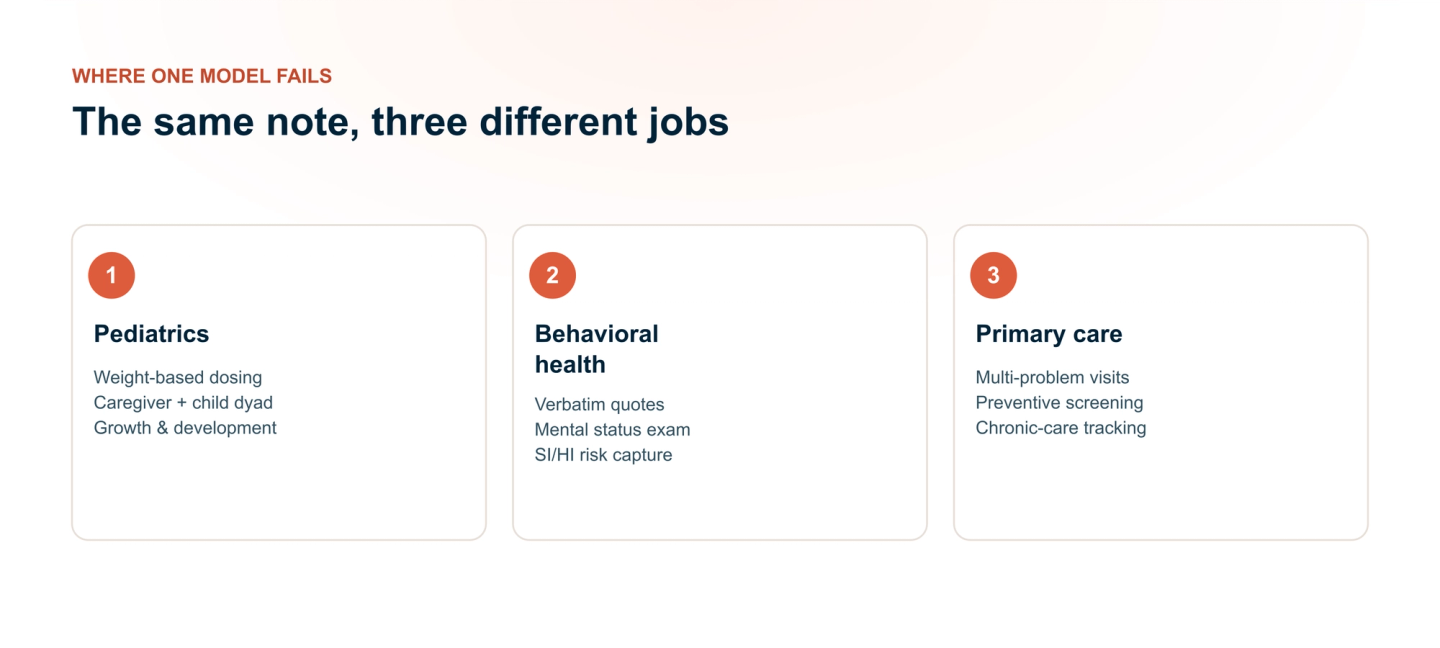
- For Pediatrics: A generic note might simply state "child appears healthy." This fails to capture critical developmental highlights like "walks independently," "uses 2-3 word phrases," or "responds to name." Such omissions can delay early intervention for developmental delays.
- For Behavioral Health: A generic note might compress the patient's narrative into a few bland sentences. It misses the quality of the thought process, the intensity of the affect, or the specificity of the cognitive distortions, all of which are diagnostically essential.
- For Primary Care: A generic note might list lab values without contextualizing them. It fails to distinguish between a stable diabetic patient and one whose A1c is rapidly trending upward
Specialization Deep Dive 1: Pediatrics
Pediatric documentation is not adult medicine on a smaller scale; it centers on growth, development, and prevention. AI that applies adult‑focused logic to children produces notes that miss critical alerts for developmental delays, vaccine gaps, or safety risks.
The Unique Demands of Pediatric Documentation
The "Parent as the Translator”
Children rarely provide their own history. AI must recognize that the Subjective section is secondhand from parents or guardians.
- AI Rule: Attribute statements correctly. Document "Mother reports fever for 2 days" rather than "Patient reports fever."
- Preserve Parent Language: Keep subjective descriptors like "fussy" or "lethargic" verbatim. Do not rewrite them into clinical jargon.
The "Growth" Imperative
The Objective section carries the heaviest weight in pediatrics. Vitals are interpretative.
- Percentiles and Trends: AI must auto-calculate weight, height/length, head circumference, and BMI percentiles.
- Screenings: AI must recognize and prompt for age-appropriate tools, such as the M-CHAT (autism) and ASQ (developmental surveillance), at designated well-child visits.
Where AI Comes In
Immunization Validation Over Listing
Generic AI simply lists vaccines. Pediatric AI must validate them.
- Action: Cross-reference the child's exact age against the CDC schedule. Flag overdue vaccines automatically and predict upcoming doses to prompt clinician discussion.
Age-Specific Guidance
The Plan section must include dynamic counseling topics tailored to the child's exact age, not a generic template.
Examples:
- Newborns = safe sleep.
- 12-month-old = choking hazards.
- Adolescents = mental health and sexual health.
AI should generate these topics automatically for clinician review.
Teen Confidentiality Handling
Adolescent visits require balancing parental access with patient privacy.
- Action: AI must flag sensitive disclosures (sexual activity, substance use, mental health) for clinician review, allowing the provider to decide what appears in the main note versus a confidential addendum.
Specialization Deep Dive 2: Behavioral Health
Unlike primary care, the Subjective narrative is the primary diagnostic tool. AI must prioritize risk detection, preserve patient voice, and structure the Mental Status Exam (MSE) with precision, all while avoiding clinical assumptions that could compromise safety or the therapeutic alliance.
Verbatim Narrative Capture
In behavioral health, how a patient says something is as important as what they say. Generic AI tends to summarize, stripping away critical clinical context.
- AI Rule: Preserve verbatim quotes and natural language patterns.
- Track Cognitive Distortions: AI should flag patterns like catastrophizing, black-and-white thinking, or thought blocking without interpreting them diagnostically.
Mental Status Exam (MSE) Structuring
The MSE is non‑negotiable in behavioral health documentation. AI must organize findings under distinct, standardized domains rather than organizing them into a paragraph.
Required Fields:
- Appearance: Grooming, dress, posture.
- Behavior: Psychomotor activity, eye contact, cooperation.
- Speech: Rate, volume, articulation.
- Mood: Patient's self-reported emotional state (e.g., "sad," "anxious").
- Affect: Clinician-observed emotional range and congruence with mood.
- Thought Process: Linear, circumstantial, tangential, loosening of associations.
- Thought Content: Delusions, obsessions, SI/HI, paranoia.
- Cognition: Alertness, orientation, memory.
- Insight & Judgment: Patient's awareness of their condition and decision-making capacity.
The Importance of Risk Management
When AI detects high‑risk keywords (suicide, self‑harm, homicide, hopelessness), its job is to flag.
- AI Rule: Never rephrase or soften risk language. Document exactly as stated and trigger an explicit visual/system alert for clinician review.
Plan Differentiation (Therapy Note vs. Crisis Plan)
AI must distinguish between a routine therapy progress note and a crisis/safety plan.
- Routine Plan: Document therapeutic modalities used (CBT, DBT), homework assigned, and next appointment.
- Crisis Plan: Must include concrete, actionable items: emergency contacts, coping strategies, warning signs, and a clear escalation pathway.
Specialization Deep Dive 3: Primary Care
Primary Care is the medical home, where chronic conditions are managed, prevention is delivered, and referrals are coordinated. AI must excel at integrating multiple data streams, organizing complex visits, and ensuring no follow‑up or referral slips are overlooked.
The Unique Demands of Primary Care
The Objective section is where synthesizing vitals, labs, imaging, and medications happens.
- AI Rule: Flag out-of-range values, highlight trends, and cross-reference with diagnoses.
Where AI Comes In
E/M Coding Precision
E/M coding relies on Medical Decision Making (MDM): problems, data reviewed, and risk.
- AI Action: Track number/severity of problems, count data points reviewed, assess medication risk. Accurately reflect complexity.
Problem-Oriented Organization
Primary care visits involve multiple active problems. AI must structure the Assessment and Plan by each problem.
Care Coordination
The Plan is a To‑Do List, and the plan section must be actionable and trackable.
- Referrals: Document specialist referrals with urgency.
- Follow-Ups: Specify exact timeframes.
- Care Gaps: Flag missing services, immunizations, or screenings.
Best Practices for Implementing Specialty-Specific AI
To maximize accuracy, safety, and clinical utility, healthcare organizations should adopt these practices when implementing AI for SOAP note generation:
1. Specialty-Specific Prompt Engineering
Customize AI prompts for each department with specialty‑specific vocabulary, templates, and required data fields.
- Pediatrics: Include growth percentiles, milestone tracking, and immunization validation.
- Behavioral Health: Structure the Mental Status Exam (MSE) with all required domains.
- Primary Care: Organize Assessment/Plan by individual problems with lab integration.
2. Mandatory Human Review
- AI generates drafts, and clinicians must review and edit before finalization.
- Never auto-approve AI-generated notes without clinical oversight.
- Human review catches hallucinations, attribution errors, and missing context.
3. Protocols Against Hallucinations
- Instruct AI to "only document what was said or observed".
- Flag high-risk language (SI/HI, abuse concerns, violence) for mandatory human review.
- Do not allow AI to rephrase or soften risk-related patient statements.
4. Regular Audits and Feedback Loops
- Conduct monthly audits of AI-generated notes for accuracy, coding compliance, and completeness.
- Establish clinician feedback rules to flag errors and continuously improve AI performance.
5. Compliance with Privacy Regulations
- Ensure AI vendors are HIPAA-compliant with executed Business Associate Agreements (BAAs).
- For behavioral health, comply with 42 CFR Part 2 (substance use records).
- Implement state-specific confidentiality protocols for adolescent-sensitive information.
Conclusion
AI has the power to transform clinical documentation, but only if we abandon the one‑size‑fits‑all approach. The distinct demands of Pediatrics, Behavioral Health, and Primary Care require AI to adapt its vocabulary, structure, and clinical focus accordingly. Organizations that invest in specialty‑specific AI will see improved documentation quality, reduced burnout, and enhanced patient safety. The choice is clear: the future of healthcare documentation is specialized, not standardized.