



The SOAP note (Subjective‑Objective‑Assessment‑Plan) has been the backbone of clinical documentation. But in today's fast‑paced, value‑based care environment, its structure is showing cracks. Overlooked assessments and delayed action plans contribute to handoff errors and clinician burnout.
That's why a growing number of health systems are now testing APSO (Assessment‑Plan‑Subjective‑Objective), a simple reordering that prioritizes clinical reasoning first. The only challenge is that most AI tools were trained on SOAP. Now, forward‑thinking AI SOAP note tools are rapidly adapting to support APSO workflows without sacrificing accuracy or compliance. Learn about what's changing, and how AI is keeping up.
The Historical Dominance of SOAP (And Its Hidden Flaws)
Introduced by Dr. Lawrence Weed in the 1960s to organize problem‑oriented medical records, the SOAP framework was revolutionary for its time, imposing structure on paper charts and enabling systematic clinical reasoning.
Why SOAP Works Well
- Start with the Patient: The Subjective (patient's story) came first because that's how a clinical encounter naturally unfolds.
- End with Action: The Plan logically concluded the note after gathering all data.
- Linear Thinking: On paper, this top-to-bottom format mimicked the sequential flow of a visit.
Three Critical Flaws Emerging in Modern Healthcare
While SOAP served paper‑based medicine well, today's digital, fast‑paced environment exposes three major weaknesses:
1. The Overlooked Lead
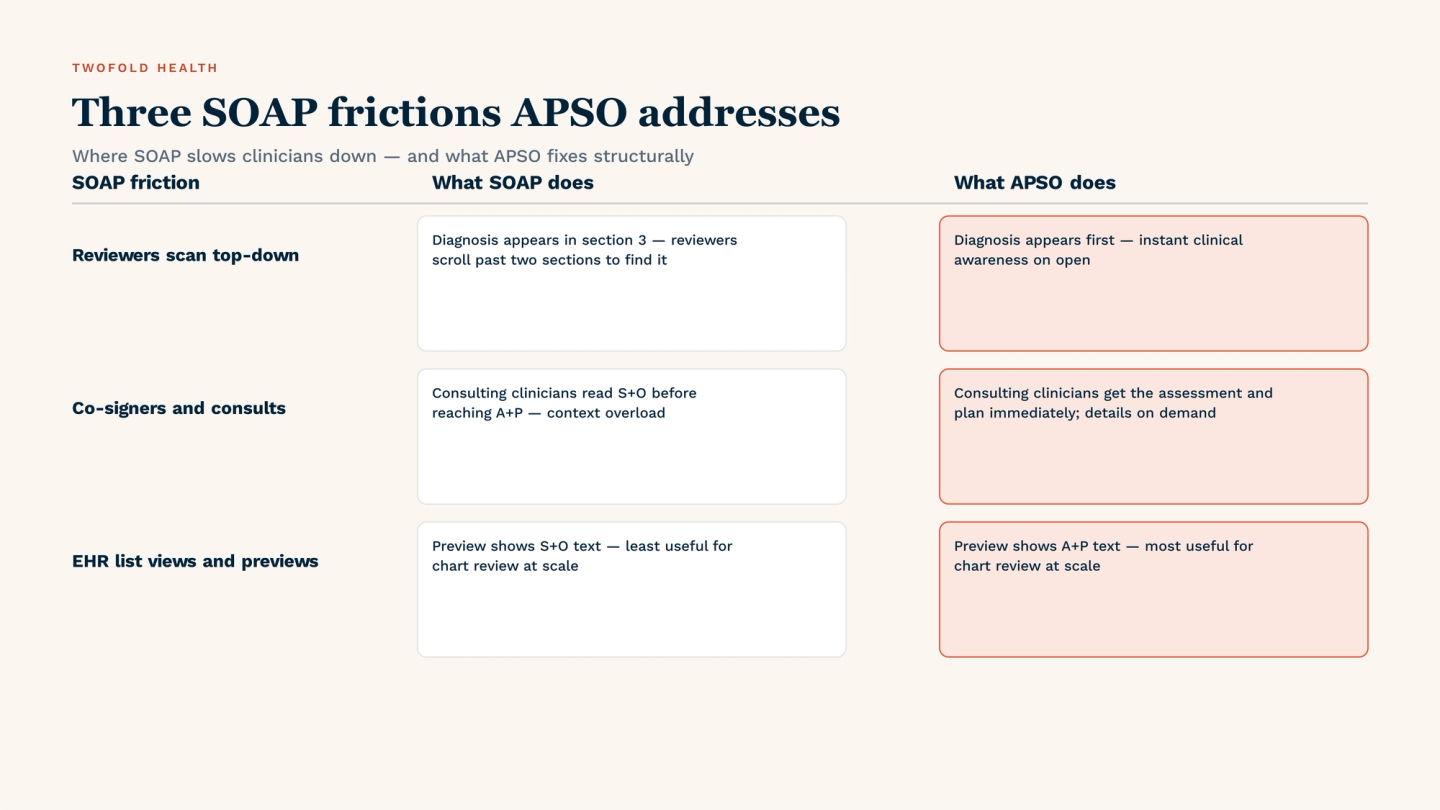
In emergency departments and urgent care, the Plan is the most urgent information for handoffs, sign‑outs, and covering physicians.
- The Problem: In a traditional SOAP note, the Plan lives at the very bottom, buried beneath Subjective narratives and Objective data.
- The Consequence: Clinicians waste time scrolling or clicking to find what they actually need.
2. Repetition Bloat
Objective data (labs, vitals, imaging results) is often auto‑populated or copied forward from previous notes.
- The Problem: This creates lengthy, redundant records where unique clinical thinking, the Assessment, gets lost.
- The Consequence: Critical diagnostic reasoning becomes harder to find. Notes grow longer but not more informative.
3. Reimbursement Mismatch
Value‑based care and medical billing increasingly prioritize Medical Decision Making (MDM), which requires clear justification of why a diagnosis was made (Assessment) before detailing what will be done (Plan).
- The Problem: SOAP delays the Assessment until after the Subjective and Objective sections.
- The Consequence: Denials and queries increase because the clinical rationale is obscured.
Introducing APSO (Assessment-Plan-Subjective-Objective)
APSO format puts the diagnosis and action plan first for handoffs, billing, and team communication. APSO also doesn't remove any information; it simply reorders the note to match clinical priority rather than chronological encounter flow.
Section | Order in APSO | Content Type |
|---|---|---|
Assessment | 1 | Clinical synthesis, diagnosis, reasoning |
Plan | 2 | Actionable steps, orders, follow-ups |
Subjective | 3 | Patient narrative, HPI, chief complaint |
Objective | 4 | Vitals, exam findings, labs, imaging |
The Key Benefit: Instant Clinical Awareness
A physician can read the first two lines (Assessment + Plan) and instantly know the clinical decision. The Subjective and Objective sections serve as supporting evidence.
Who Benefits Most from APSO?
For Covering Physicians & Handoffs:
- Critical actions (meds, consults, follow-ups) are visible without scrolling.
- Risk of missed orders decreases because the Plan is front-loaded.
- APSO aligns with how physicians are trained to think: "What is the problem, and what will I do about it?"
For Billing and Compliance:
- Medical Decision Making (MDM) is immediately visible to auditors.
- Justification (Assessment) directly precedes action (Plan); ideal for prior authorization and appeals.
- Reduced denial rates for services requiring a clear clinical rationale.

How AI Is Adapting to APSO Workflows
The shift to APSO requires AI to rethink how it prioritizes clinical information.
The Main AI Adaptation for APSO
Dynamic Section Reordering (No Retraining Required)
- How it Works: Modern AI scribes now offer configurable output templates. Instead of retraining the model on APSO-specific data, the AI generates a complete structured note following the APSO format.
Key Advantage:
- Preserves AI accuracy (models are still optimized for SOAP generation).
- Gives clinicians flexibility (toggle between SOAP and APSO views).
- No data loss; all four sections remain fully intact.
What AI Still Gets Wrong in APSO
- Some AI models cut essential context from Subjective when trying to be "brief."
- AI may rephrase the chief complaint instead of providing a true clinical synthesis.
- Always review AI-generated APSO notes before signing.
Practical Steps for Switching to APSO (With AI Assistance)
Moving from SOAP to APSO requires workflow changes, team alignment, and AI configuration. The table below outlines a tested 5‑step implementation checklist for practices considering the switch.
Step | Action |
|---|---|
1 | Audit your current SOAP notes to understand why you want to make the switch. |
2 | Train your AI scribe with custom instructions/specialty-specific prompts. |
3 | Start with a pilot team (low-risk, high-speed specialties). |
4 | Update your EHR templates and display logic. |
5 | Train your team on APSO-specific documentation habits. |
Conclusion
APSO doesn't ignore decades of documentation structure; it simply reorders priorities to match how clinicians actually think and hand off care. AI has proven to be agile in this transition, learning to extract decisions and reorder output without sacrificing accuracy. The result is fewer handoff errors, and notes that respect the clinicians' time. Change is never easy in healthcare, but sometimes the smallest rearrangements yield the biggest gains.