



Documentation demands significantly impact clinical efficiency and satisfaction. Traditional EHR notes, primarily narrative text, resist automated analysis, limiting their utility beyond immediate reference. However, artificial intelligence introduces a solution. By converting unstructured dictations into categorized data elements, AI enables seamless interoperability across systems. This transformation supports clinical decision‑making, automates administrative tasks, and generates concise summaries. Explore how integrating structured AI clinical notes can enhance workflow efficiency and shape the future of clinical workflows.
From Dictation to Data: The Shift to Structured AI Clinical Notes
Traditional narrative notes capture important context, but their format makes them hard to search and process automatically. This unstructured format obstructs predictive analytics, quality reporting, and accurate risk‑adjustment coding (e.g., HCC capture), often resulting in billing inaccuracies and missed clinical insights.
The AI Structuring Mechanism
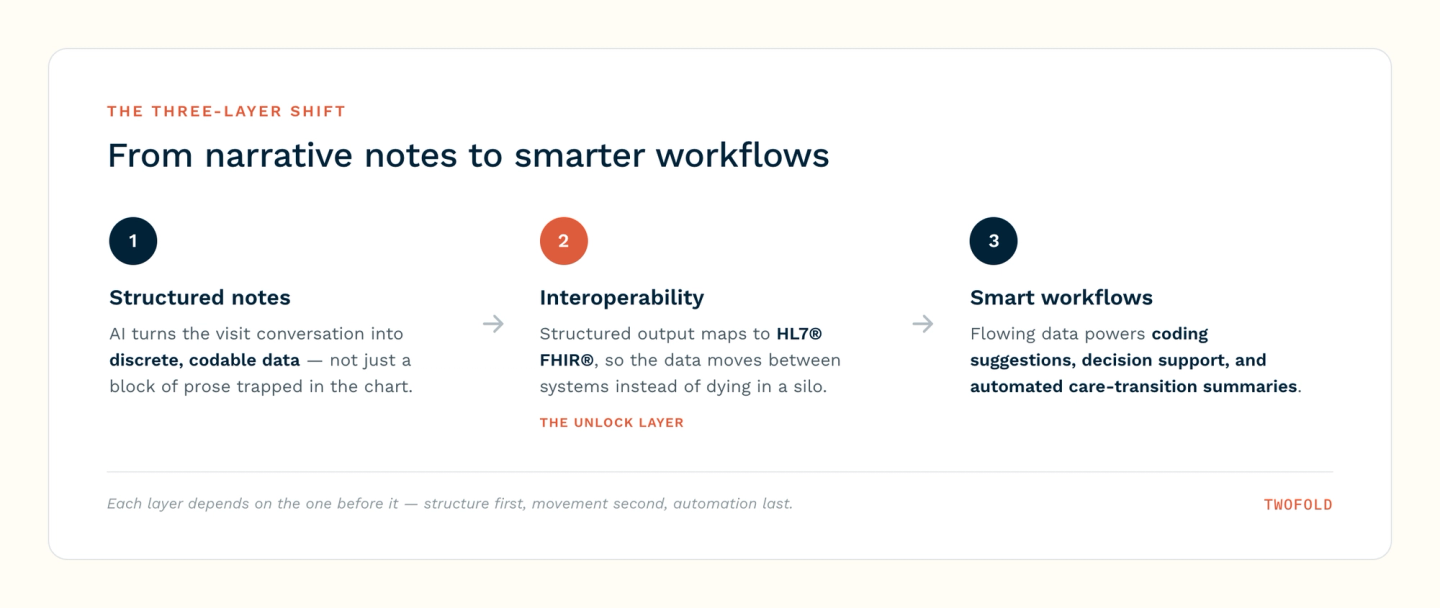
Fine‑tuned Natural Language Processing (NLP) models extract clinical entities such as symptoms, medications, and diagnoses from dictations. These entities are mapped to standardized ontologies, including SNOMED CT, and subsequently populate predefined EHR fields.
Interoperability: The Key to Smarter Workflows
Structured AI clinical notes lose significant value if they remain trapped within a single Electronic Health Record (EHR). Interoperability, the secure exchange of patient data across systems, settings, and stakeholders, transforms these data points into a continuously updated, system‑wide clinical asset.
FHIR as the Foundational Standard
The structured output generated by AI notes aligns directly with HL7® FHIR® (Fast Healthcare Interoperability Resources). By mapping SNOMED‑coded diagnoses and RxNorm‑coded medications to FHIR profiles, clinical data becomes transportable across disparate EHR platforms (e.g., Epic, Cerner, Meditech).
Breaking Down Clinical Silos
Without interoperability, specialists operate with incomplete information. With structured, FHIR‑enabled notes, care transitions improve.
- Reduced Redundancy: Current structured data prevents duplicate orders for imaging or laboratory tests, reducing both costs and patient inconvenience.
- Closed-Loop Referrals: Referral notes contain structured data on specific questions, ensuring the specialist addresses the exact clinical concern.
Enabling Clinical Decision Support (CDS) at Scale
Interoperability creates a bidirectional data stream that amplifies CDS capabilities.
- Cross-System Alerts: Structured data ingested from an external Emergency Department visit can trigger an alert within the primary care EHR about a new allergy or contraindicated medication.
- Population Health Dashboards: Aggregated structured data across interoperable networks enables real-time monitoring of disease prevalence, quality metrics, and care gaps.
The "Smart" Workflow: Automation and Actionable Insights
Once AI structures clinical data and interoperability enables its flow, the clinical workflow shifts from passive documentation to proactive structuring. The structured note becomes a trigger for automated tasks and intelligent decision support.
AI-Assisted Coding and Revenue Cycle Management
Structured data directly maps to billing requirements, reducing manual abstraction and retrospective audits.
- ICD-10 and CPT Suggestion: The AI cross-references documented diagnoses and procedures with medical necessity criteria, suggesting appropriate codes at the point of documentation.
- Risk Adjustment Capture: Structured extraction of chronic conditions (e.g., diabetes with complications) improves Hierarchical Condition Category (HCC) accuracy, ensuring complete reimbursement.
- Claim Integrity: Automated validation flags mismatches between diagnosis codes and documented clinical indicators before claim submission.
Summarization for Care Transitions
Structured data enables concise summarization, critical during shift changes or transfers.
- Automated Discharge Summaries: The AI distills structured problem lists, medication reconciliations, and pending labs into a standardized handoff document.
- Specialist Referral Briefs: The primary care note is condensed into a structured list, allowing the specialist to review only relevant clinical context.
- Actionable Next Steps: The system generates a structured care plan indicating pending orders, follow-up dates, and unresolved clinical questions.
Challenges and Considerations in AI Adoption
Despite the promise, several structural and technological barriers must be acknowledged and addressed for safe implementation.
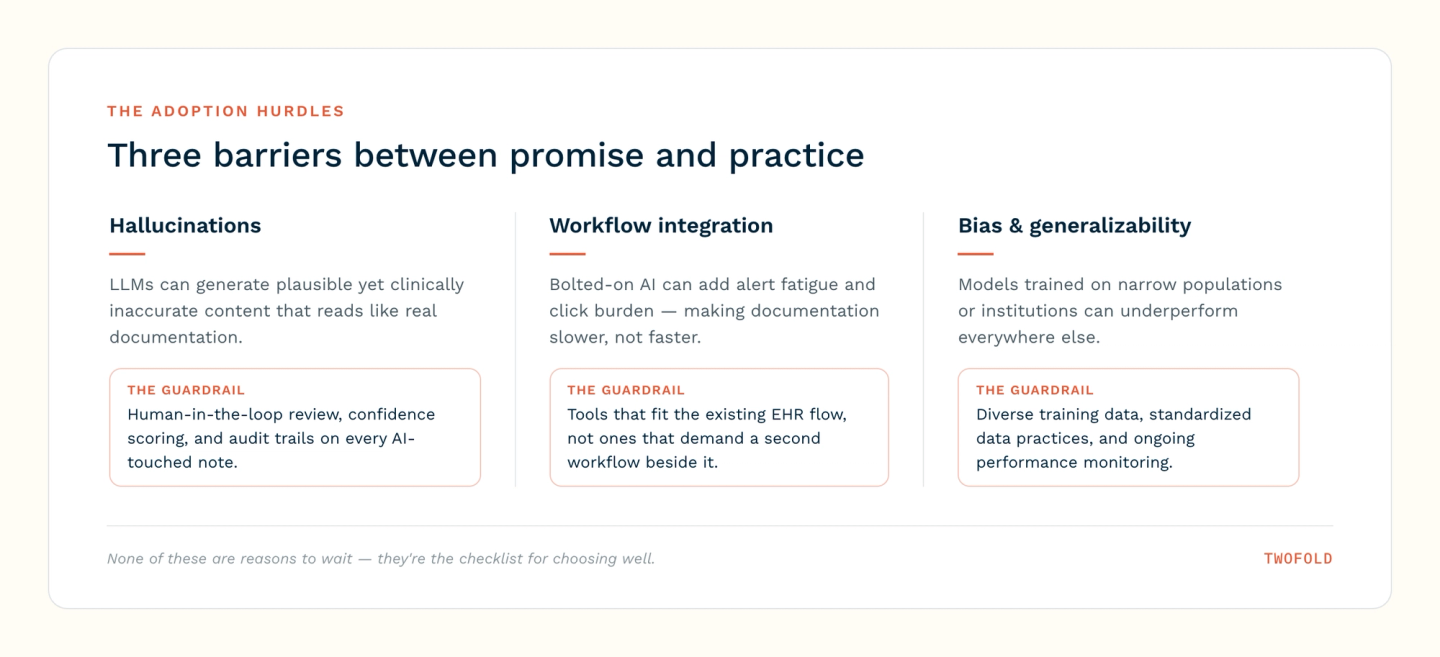
Algorithmic Hallucinations and Clinical Fidelity
Large language models may generate plausible yet clinically inaccurate content called hallucinations, including fabricated medications or misinterpreted symptoms.
- Human-in-the-Loop: All AI-generated structured fields require clinician validation before integration into the permanent record.
- Confidence Scoring: AI should output confidence intervals for each structured entity, flagging low-certainty extractions for mandatory human review.
- Audit Trails: Systems must log all AI-suggested changes, enabling error tracking and model refinement.
Workflow Integration
Introducing AI tools into existing EHR environments can increase documentation time if the user experience (UX) is poor.
- Alert Fatigue Risk: Poorly tuned Clinical Decision Support can overwhelm clinicians if the frequency is excessive.
- Click Burden: If clinicians must toggle between dictation, structured fields, and validation panels, efficiency gains will decrease.
- Solution: AI outputs should be presented as drafts within the existing note interface, allowing single-click acceptance or editing.
Bias and Generalizability
AI models trained predominantly on data from specific populations or institutions may underperform across diverse patient demographics.
- Data Source Limitations: Training corpora often overrepresent tertiary care centers and specific geographic regions.
- Standardized Data Gaps: Social determinants of health (SDOH) are inconsistently captured in structured formats, limiting equitable risk adjustment.
- Mitigation: Organizations should evaluate model performance on their local patient population and consider fine-tuning with institutional data.
What's Next for AI Clinical Notes
The table below outlines key emerging capabilities for the AI clinical note workflow:
Field | Emerging Capability |
|---|---|
Predictive Analytics | AI leverages structured historical data to generate real-time risk scores |
Learning & Privacy | AI models train across institutional datasets without exposing protected health information, preserving patient privacy. |
Conclusion
Structured AI clinical notes are transitioning from concept to clinical reality, driven by advances in NLP, FHIR interoperability, and predictive analytics. When fully realized, these systems will automate administrative tasks, provide actionable insights, and enable population‑level research while maintaining patient privacy. Realizing this potential requires addressing algorithmic bias, integration challenges, and governance frameworks. Ultimately, the future of AI clinical documentation is about equipping clinicians with intelligent tools that enhance safety, efficiency, and evidence‑based decision‑making.