



It is 9:40 p.m. The kids are down. The clinic closed seven hours ago. A solo mental‑health clinician in Colorado — we'll call her Dr. L. — is still at the kitchen table finishing notes from a full day of therapy and medication‑management visits.
This is the part of the job no one warned about in training. The visits ended hours ago. The charting did not. Mental status exams, risk language, the rationale behind every treatment decision — all of it has to be reconstructed from memory while it slowly fades. By the time the last note closes, it is nearly 10 p.m., and tomorrow's first patient is at 8 a.m.
That nightly catch‑up is not a personal failing. Clinicians spend close to 5.9 hours a day in the EHR, and roughly 90 minutes of it lands after hours — the stretch researchers named “pajama time” (Arndt et al., Annals of Family Medicine). For Dr. L., pajama time had quietly become a second shift: about 110 minutes of charting every night after the family was asleep.
Ninety minutes a night is not a rounding error. It is most of a working day, handed back every single week. Then the math changed. Here is what actually happened — numbers and caveats included.
Below: the exact before‑and‑after, why earlier fixes failed for mental health specifically, the day‑one workflow, and a straight FAQ on HIPAA, accuracy, EHRs, and price.
The numbers, and where they came from
Figure | Value | Source |
|---|---|---|
Nightly charting before Twofold | ~110 min | This clinician |
Nightly charting after Twofold | ~20 min | This clinician |
Time back each night | ~90 minutes | 110 min minus 20 min |
Time to generate a note | Under 60 seconds | Twofold product docs |
First note after signup | Within ~10 minutes | Twofold onboarding |
Visit length captured | Up to 1.5 hours per session | Twofold product docs |
Twofold figures are from trytwofold.com and the Twofold Help Center. The case figures are this clinician's own before‑and‑after; her identity is anonymized at her request.
What charting looked like before, and why two “fixes” failed
The backlog was not from slow typing. It was structural. Mental‑health notes carry weight that a generic template does not: a mental status exam, a risk assessment, the clinical reasoning behind a treatment or dose change. Reconstructing all of that hours later, from memory, is the slow part.
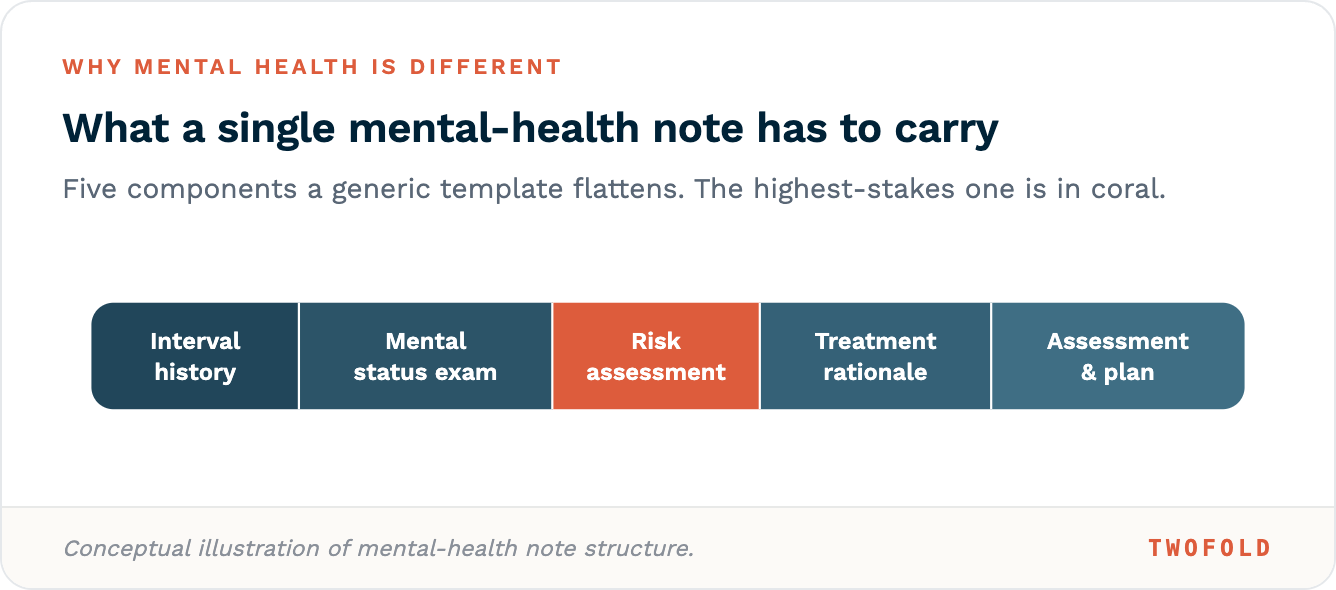
The slow part was never typing speed. It was rebuilding the highest‑stakes parts of the note from memory, hours after the room went quiet.
This is not unique to one clinician — when private‑practice providers are asked what fuels burnout, documentation lands at or near the top (Tebra, The Intake). But the industry average is not the point of this piece, and it is not why you would cite it. The point is one real clinician's before and after, which has no other home on the internet.
So Dr. L. tried the obvious tools first. Both fell short for mental health in specific ways.
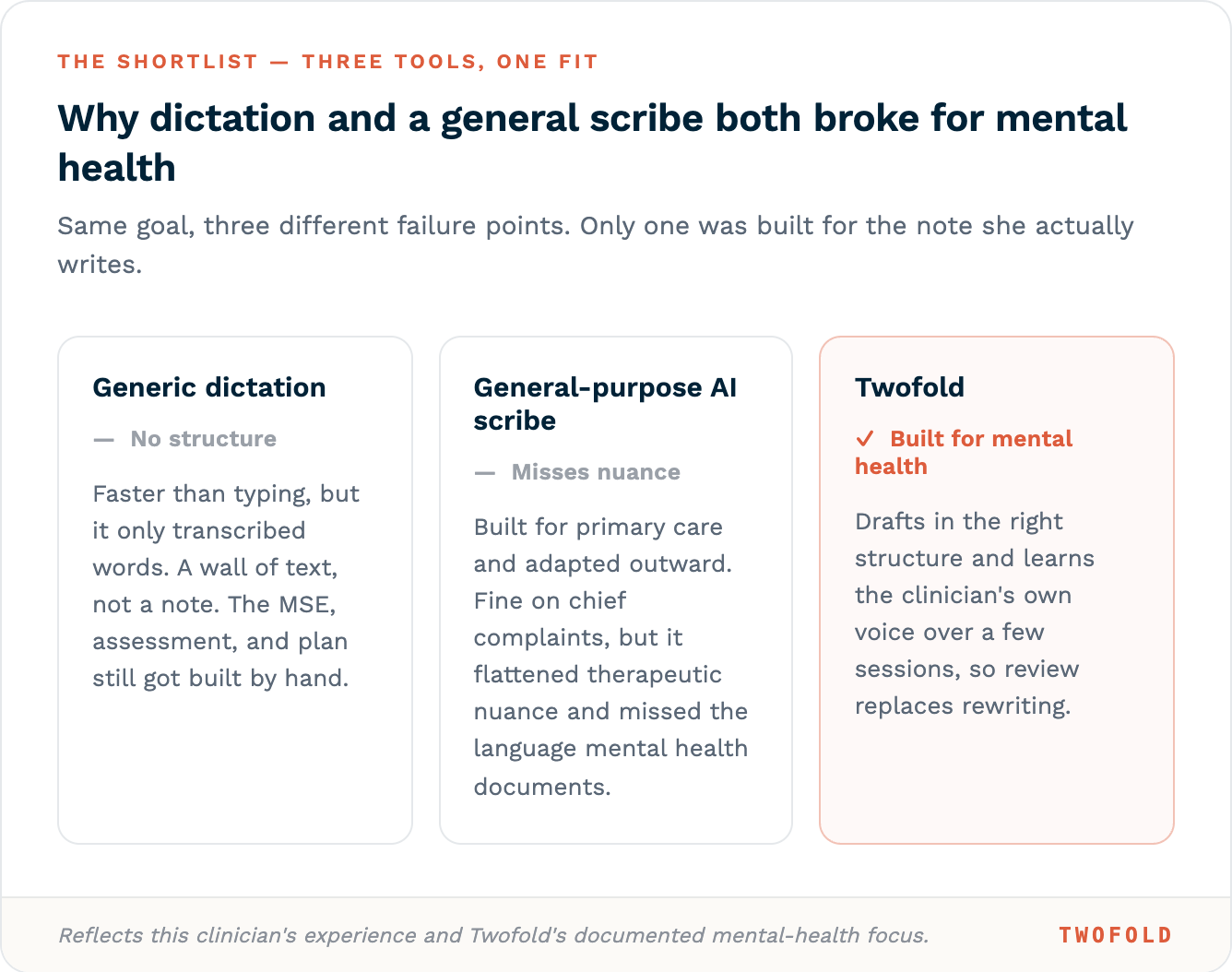
A scribe built for primary care is not a scribe built for mental health. The note is a different shape, and the shape is the whole job.
The switch, and the skeptical first week
Adoption was not a leap of faith. Setup took about five minutes: sign up, agree to the terms and the Business Associate Agreement (which is executed automatically at signup), pick the clinician type, and run a quick demo script that generates a sample note in real time. The first real note came within roughly ten minutes.
The first week was spent not trusting it. That is the right instinct. Dr. L. read every generated note line by line against her memory of the session, watching for what it would miss on risk language and treatment rationale. The convincer came about thirty notes in, near the end of the first week. A patient had mentioned passive suicidal ideation almost in passing, and the draft had already pulled it into the risk section and reflected the safety plan she had talked through in the room, worded close to the way she would have written it herself. After that she stopped re‑typing notes and started reviewing them.
The workflow itself is three steps, and it is the same whether the visit is in person or over telehealth.
Three taps during the visit replace an hour of reconstruction after it.
The finished note gets pasted into SimplePractice, the EHR Dr. L. runs her practice on. Twofold does not plug directly into the EHR, which sounds like a downside and mostly is not — it means the workflow layers onto any system without an integration project. More on that limit below.
The result: about 90 minutes back, every night
The change showed up where it mattered, in the evening. Nightly charting dropped from about 110 minutes to about 20. Notes now get finished the same day — often between sessions, while the visit is still fresh — instead of being reconstructed at the kitchen table at night.
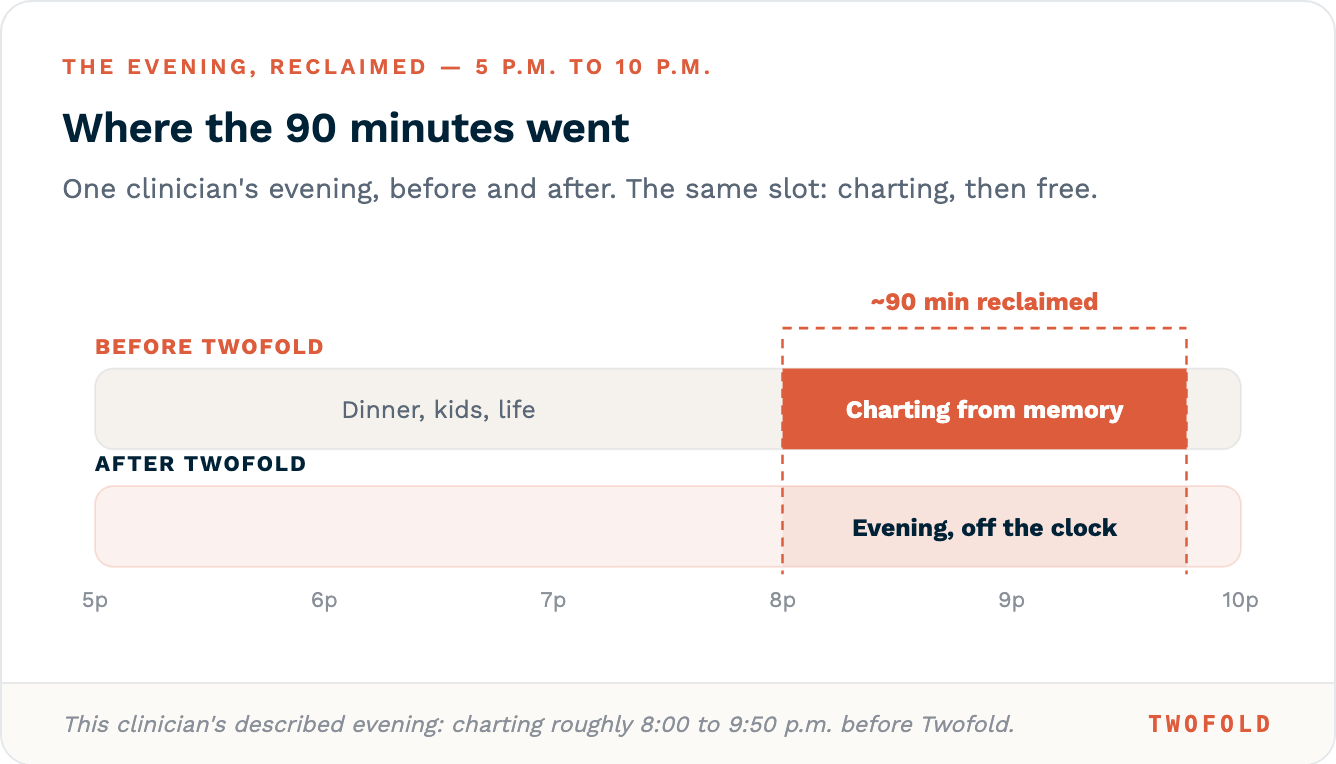
The charting block did not get faster. It moved off the clock entirely.
Randomized trials of ambient AI scribes point the same direction (UW Health; UCLA, NEJM AI 2025): less documentation time, lower burnout, with the size of the win varying by clinician and tool. That research is useful corroboration, and it has a hundred other homes. The number that actually matters here is this clinician's own: about 110 minutes a night down to about 20.
The honest limits: what it did not fix, and who should skip it
An AI scribe is a first draft, not a final note. This matters more in mental health than almost anywhere, because the stakes of a missed risk statement are real. Here is the straight version.
It still needs your review, every time. Twofold drafts; the clinician is accountable for accuracy. Catching an error in a draft is faster than writing from scratch, but it is not optional — especially for risk language and treatment rationale.
There is no direct EHR integration. You copy and paste the finished note. For most solo and small practices that is fine and even an advantage, since it works with any EHR. If you want a note that posts itself into the chart automatically, this is not that.
It has to stay open while capturing. Per Twofold's own docs, if the app closes or the screen goes dark mid‑visit, the session may not capture correctly. The full transcript view is currently desktop only.
It depends on consent. Recording requires the patient's verbal consent, and Twofold supplies a sample script. Patients who decline recording can still be documented through the dictation or upload paths, but the hands‑off ambient experience assumes a recorded visit.
Who should skip it: practices that need deep bidirectional EHR integration today, settings where patients routinely refuse any recording, and large organizations that need enterprise SSO and admin controls as a hard requirement (though a group plan with an org‑wide BAA does exist).
And to be clear about what it did not solve for Dr. L.: it drafts the clinical note, but it does nothing for the insurance and billing side — the superbills, prior authorizations, and claim follow‑ups that still cost her a few hours most weeks. The evenings came back; the reimbursement paperwork did not go anywhere.
How your data is handled
Twofold is HIPAA and HITECH compliant, and a Business Associate Agreement is executed automatically when you sign up. Audio is processed in real time, never stored on disk, then deleted once the note is generated. Data is encrypted in transit and at rest, hosting runs on Microsoft Azure under a BAA, and patient data is never used to train AI models. For the longer version, see how AI scribes handle HIPAA and patient data.
Want to see it on your own notes? Twofold has a free 7‑day trial, no credit card, and you can generate your first real note in about ten minutes. Start with Twofold free.