



Brief Answer
With true back to back fifteen minute visits, you have three realistic options: build micro gaps into the schedule, document inside the encounter, or use an AI assistant so most of the note is drafted by the time you close the chart. For most clinicians, a mixed approach works best: a brief in room capture or dictation, a short protected block mid session or at the end of a cluster, and a simple repeatable template so each note takes only a few minutes to finalize. AI scribes can help, but they must fit your timing, be HIPAA eligible, and still leave you in control of the final wording.
The Longer Answer
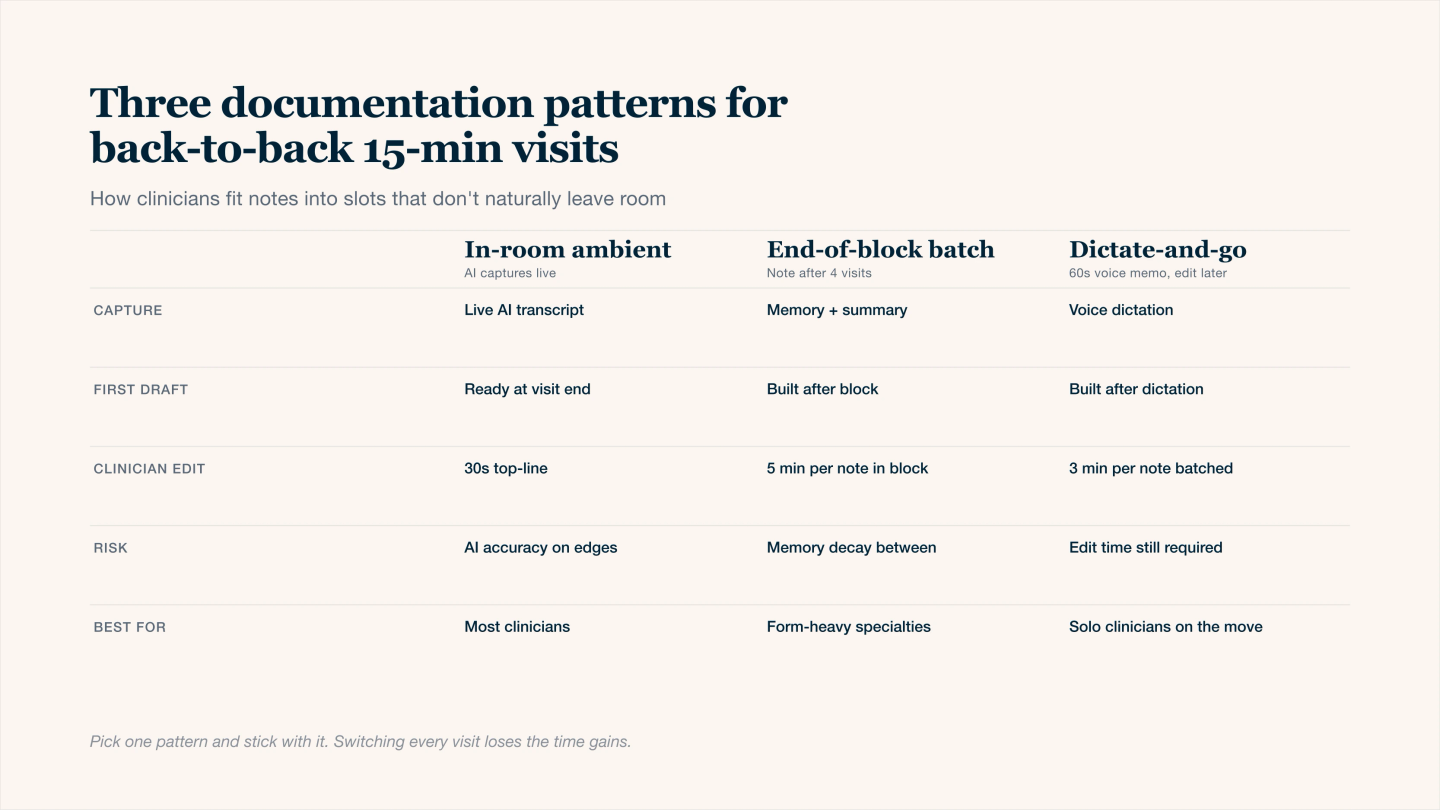
Three documentation patterns for back-to-back 15-min slots — pick one and stick with it.
1. First reality check
If you have fifteen minute slots with no gaps at all, there is no hidden magic time. Notes only happen if you:
- Do some documentation during the encounter itself
- Create small buffers between visits, even two to three minutes
- Or use a tool that drafts most of the note while you focus on the patient
So the question becomes less “when” and more “what is the least disruptive way to embed note writing into a continuous clinic session”.
2. Common documentation patterns that do work
Most clinicians fall into one of these patterns or a combination:
Pattern | When you write | Pros | Cons |
|---|---|---|---|
In room typing | While patient talks or during review | Very fast completion, note is done at visit end | Can affect rapport, hard for sensitive topics |
Micro gap notes | Two to four minutes after each visit | Protects connection in room, note still fresh | Requires scheduling or self enforced pauses |
Cluster blocks | Short block after every three to four patients | Efficient batching, mental reset | Risk of falling behind if one case runs long |
AI assisted | AI drafts from audio or summary, you finalize later in day | Less manual typing, consistent structure | Needs good prompts and strict review habit |
You can combine them. For example, capture high level points in room, then use a five to ten minute block every three or four patients to finalize several AI drafted notes.
3. What your note actually must contain
Even in a fifteen minute visit, the note does not need to be long. It needs to be clear.
At minimum, primary care notes usually need:
Element | Why it matters | One line example |
|---|---|---|
Reason for visit | Shows why today needed a visit | “Follow up HTN and T2D, review labs.” |
Focused HPI | Links symptoms to conditions and risk | “Home BP 150s, no chest pain or dyspnea.” |
Exam highlights | Supports decisions and billing | “Lungs clear, no edema, regular heart sounds.” |
Data reviewed | Shows decision support | “Reviewed A1c 8.2, CMP normal.” |
Assessment and plan per problem | Core of medical decision making | “HTN above goal, increase lisinopril, BMP 2 wks.” |
Patient instructions and follow up | Safety, adherence, quality | “Check home BP log, return 4 weeks, ED for chest pain.” |
If your AI tool can reliably generate this structure from a short capture, your work shifts from writing to correcting.
4. Three example day structures for fifteen minute visits
You can adapt these so they match your clinic rules.
Model A: Always in room plus short end of session block
- In room: you narrate a thirty second summary near the end of each visit
- AI or template turns that into a structured note
- At the end of a two to three hour session, you take fifteen to twenty minutes to finalize all drafts in one batch
Model B: Micro gaps built into schedule
- Ask for a two to three minute buffer added to every second or third appointment
- Immediately after the visit, you open the chart, confirm key fields, sign, then move on
- You protect those micro gaps and do not convert them into more visits
Model C: Mixed plus “no carry home” rule
- In room: jot or dictate only the essential clinical decisions
- Mid session: one ten to fifteen minute block to finish any remaining notes from the morning
- End of day: another short block with the goal that no note leaves the building unstarted
The constant across all three models is that you decide in advance where documentation lives, rather than hoping it will fit “later”.
5. Making AI scribes actually usable in fifteen minute slots
To work in a fast schedule, an AI scribe or assistant should:
- Start quickly, with minimal extra clicks at visit start
- Produce notes in your preferred format, not a random essay
- Be safe for PHI (HIPAA alignment and a written BAA)
- Let you see and edit each section easily, then copy or send into your EHR
Your part is to give it focused input. That can be:
- A short spoken summary at the end of the visit
- Room audio with clear expectations about what the note should emphasize
- A quick checklist style input (problems, key findings, decisions, orders)
You still own the final note. The AI is a time saver, not a substitute for clinical judgment.