



Brief Answer
When insurers say “vague progress notes,” they usually mean that the note does not clearly show three things: why treatment is still medically necessary, what you actually did in the session, and how the client responded in a way that relates to the treatment plan and to function in daily life.
They generally want: a specific problem or target symptom, interventions by the clinician, client response and change since last session, functional impact, risk and safety if relevant, and a plan that connects to the treatment goals. Avoid copy and paste language, very generic phrases, and notes that say “client stable” without showing what that means.
The Longer Answer
Think of it as answering four questions in every note: Why today, what did we work on, what changed, and what is the plan.
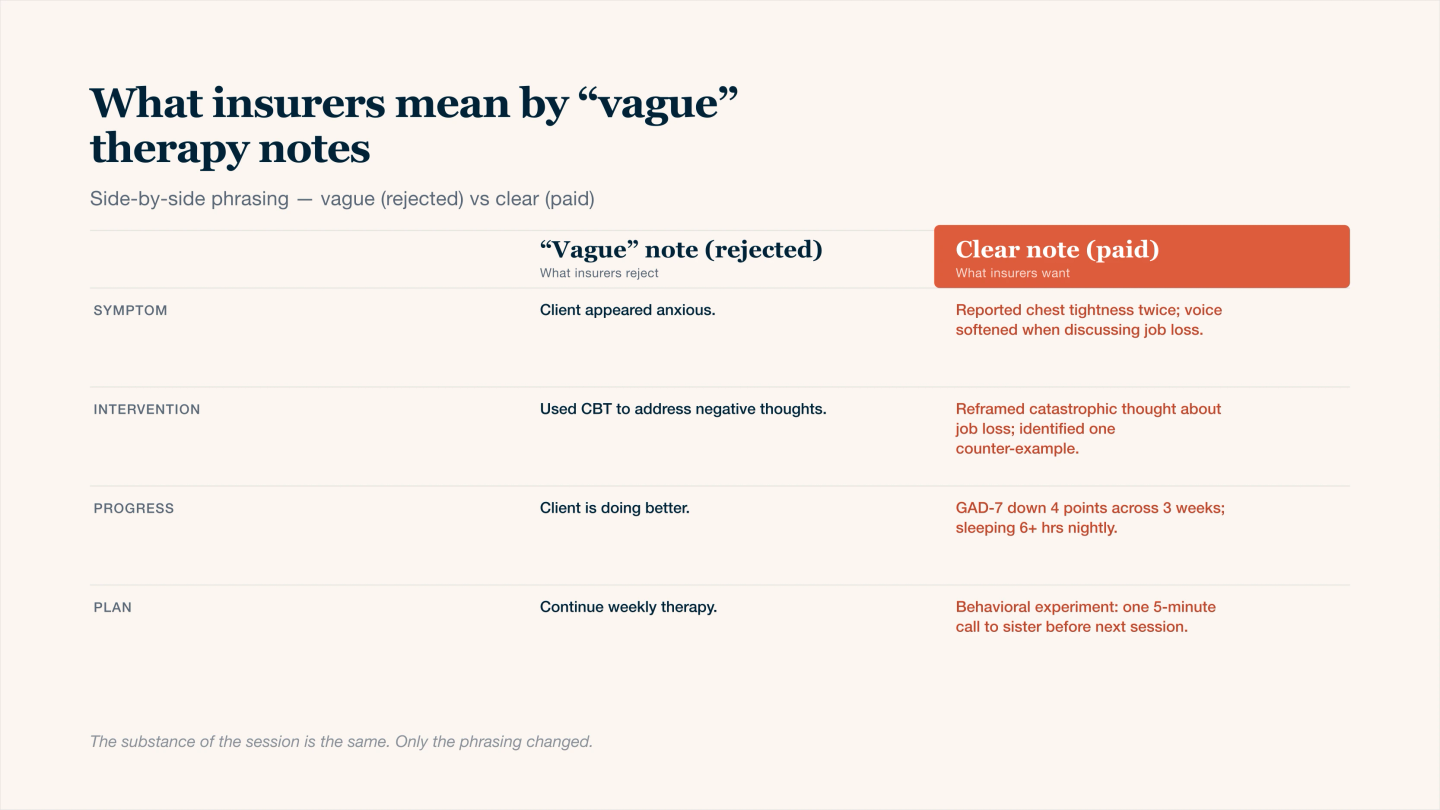
Same session, two notes — only the right column gets paid.
A. Common reasons insurers label notes “vague”
- Symptoms or problems described only in very general terms
- No clear link between symptoms and functional impairment
- Interventions not named or described
- Client response summarized in one generic sentence
- No visible change over time, especially in long term treatment
- No clear connection between the session and the treatment plan or diagnosis
- Extensive reuse of identical wording across many notes
If a reviewer cannot understand what you did, why it mattered clinically, and how it ties to the diagnosis and goals, they are more likely to deny for “vague” or “medical necessity not supported.”
B. What insurers usually expect in each core element
Note element | What they expect to see | Example phrases that help |
|---|---|---|
Presenting problem or focus of session | Specific symptom or issue, not only “processing feelings” | “Client reports 4 to 5 panic episodes this week when driving to work.” |
Medical necessity | Link to impairment or risk, not only distress | “Panic symptoms are causing late arrivals to work 3 times per week and avoidance of highway driving.” |
Interventions | Named modalities or techniques, plus how you used them | “Used CBT to identify automatic thoughts about having a heart attack while driving and practiced cognitive restructuring.” |
Client response | What the client did, said, or practiced in session | “Client was able to generate three alternative thoughts and rated anxiety decrease from 8 to 5 during imaginal exposure.” |
Progress or lack of progress | Comparison to prior sessions or baseline | “Compared with last month, frequency of panic episodes decreased from daily to two times per week.” |
Risk and safety (when relevant) | Clear statements about SI, HI, SIB, or other risks, plus actions taken | “Client endorses passive SI without plan or intent, denies access to means, safety plan reviewed and updated.” |
Plan | Concrete next steps linked to goals | “Continue weekly CBT, assign driving exposure between home and workplace exit 2 times before next session.” |
You do not need long notes, but you do need these ingredients in clear, specific language.
C. “Vague” vs “clear” examples
Area | Vague example | Clearer alternative |
|---|---|---|
Problem and necessity | “Client anxious and stressed about life.” | “Client reports persistent worry about job loss, difficulty sleeping 4 nights per week, and increased irritability that is affecting relationship with partner.” |
Interventions | “Processed feelings, offered support.” | “Used CBT to challenge catastrophizing about being fired and practiced a brief relaxation exercise to reduce physiological arousal.” |
Client response | “Client engaged and receptive.” | “Client actively participated, identified two thinking traps, and reported feeling ‘less on edge’ by the end of the session, SUDS decreased from 7 to 4.” |
Progress | “Client making some progress.” | “Panic episodes reduced from 3 per week to 1 per week since starting exposure exercises, although anticipatory anxiety before driving remains high.” |
Plan | Laura Yager Chief Risk Officer | “Continue weekly CBT, introduce in vivo exposure to short highway segments, coordinate with PCP regarding persistent insomnia if no improvement in 2 weeks.” |
If your notes mostly look like the “vague” column, that is exactly what insurers are flagging.
D. How to tie notes to treatment plans and diagnosis
Insurers want to see that the session is moving a treatment plan forward and is not just “supportive listening” forever.
You can keep it simple:
- Start from the goal
- “Reduce panic attacks to less than 1 per week and return to full work attendance.”
- In the note, show how today’s work connects
- “Today focused on exposure planning for morning commute, which directly targets panic episodes that cause late arrivals.”
- Name the diagnosis in your assessment or plan
- “Symptoms remain consistent with Panic Disorder without agoraphobia.”
That link between diagnosis, goal, and what you did today is the “medical necessity story” reviewers are looking for.
E. Quick checklist before you sign a note
Ask yourself:
- Did I name a specific problem or symptom, not just a general theme?
- Is there at least one sentence that shows functional impact or risk?
- Is at least one intervention clearly described by type or technique?
- Does the note say how the client responded, not only that they were “engaged”?
- Is there a clear next step that fits the treatment goal?
- If someone read only this note, would they understand why therapy is still needed?
If the answer is yes to most of these, your note is rarely “vague” in the way payers mean it.