



Brief Answer
Standardize your structure (problem‑oriented A/P), capture a 30–60s summary at the end of each encounter, and let AI draft the skeleton while you only confirm meds, decisions, monitoring, and follow‑up. Keep each problem to one tight assessment line + 3–4 plan bullets tied to today’s data and goals. This usually reduces after‑hours charting to a brief end‑of‑clinic sweep.
The Longer Answer
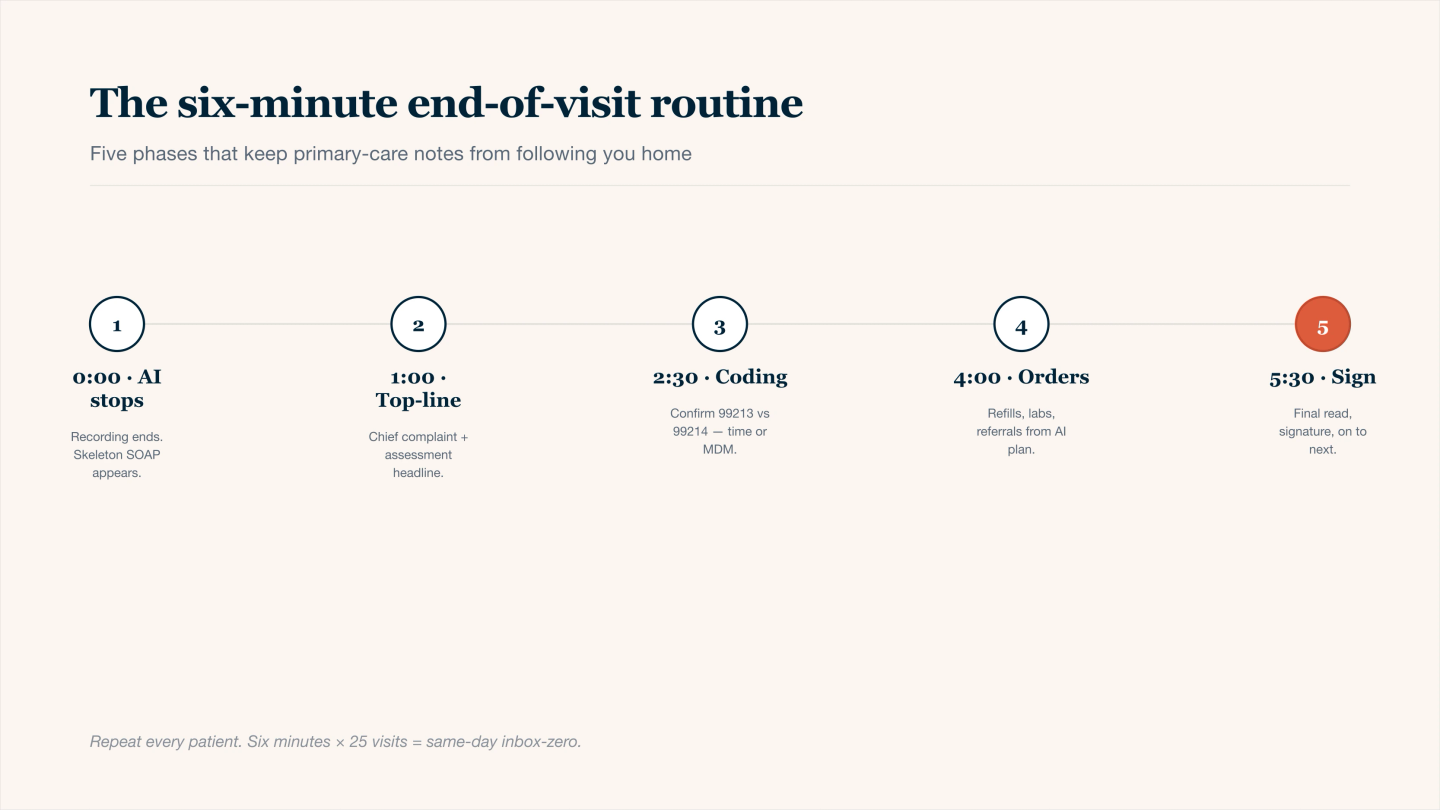
The six-minute end-of-visit routine — repeat every patient, evenings stay free.
1) Six-minute end-of-visit routine (repeat every patient)
Minute 1 – Snapshot: List today’s problems (e.g., HTN above goal, T2D fair control, URI).
Minute 2 – Findings: Dictate only salient Hx/PE changes (home BP, foot exam, red flags).
Minute 3 – Data: State data reviewed/ordered (A1c, CMP, microalbumin, X‑ray).
Minute 4 – Decisions: Meds started/continued/uptitrated; monitoring (labs, vitals).
Minute 5 – Counseling & risk: 1–2 lines lifestyle + return precautions.
Minute 6 – Follow-up & tasks: Concrete timeframe; referrals; patient instructions (3 bullets).
Feed that 30–60s audio (or typed bullets) to your AI tool; edit the draft in under 2–4 minutes.
2) Problem-oriented note skeleton (copy once; reuse forever)
- CC & Problems Today: “HTN above goal, T2D suboptimal, knee OA flare.”
- Salient Hx/PE: “Home BP 150s; A1c 8.2; knee effusion; no red flags.”
- Data Reviewed/Ordered: “Reviewed A1c; ordered CMP/microalbumin; PT referral.”
- Meds/Reconciliation: “Continue metformin; add GLP-1; uptitrate lisinopril; topical NSAID.”
- A/P (per problem):
- HTN: “Above goal → uptitrate; home BP log; BMP 2–4 wks; FU 4 wks.”
- T2D: “Add GLP-1; A1c 3 mos; hypoglycemia education; microalbumin, foot exam.”
- Knee OA: “Topical NSAID; home PT; activity mod; imaging if no improvement; FU 6–8 wks.”
- Counseling & Risk: “Diet/weight goals; return for CP/SOB, fever >101.5, calf swelling.”
- Patient Instructions: “1) Track BP daily, 2) Start GLP-1 per instructions, 3) Knee exercises x5/wk.”
- Follow-up: “4 wks (BP), 6–8 wks (knee), 3 mos (A1c).”
3) Prompts that consistently produce concise, audit-ready drafts
- Visit cue: “Primary care med-mgmt. Problems: [list]. Salient Hx/PE: [ ]. Data reviewed/ordered: [ ].”
- Per-problem A/P: “For [problem]: status [ ], goal [ ], plan [med/dose/tests/referral], rationale [ ], FU [ ].”
- Instructions & risk: “3 patient instructions + return precautions in one line.”
4) Do this, not that (to protect time and coding)
- Do anchor medical necessity to today: symptoms or quality gaps (e.g., A1c above goal).
- Do name data reviewed/ordered explicitly.
- Do keep each problem to 1 assessment line + 3–4 bullets.
- Don’t paste cloned A/P; rotate wording and include current vitals/goals.
- Don’t bury decisions in paragraphs—make them scannable bullets.
5) Quick coding cues (99213 vs 99214; time or MDM)
- Support MDM with problems (number/complexity), data (review/ordering), and risk (med changes, monitoring).
- If billing by time, record total time and what it included (review, counseling, documentation).
- Add preventive/acute items as their own problem blocks to stay clean and defensible.